IntraLock mini implant: what is causing paresthesia?
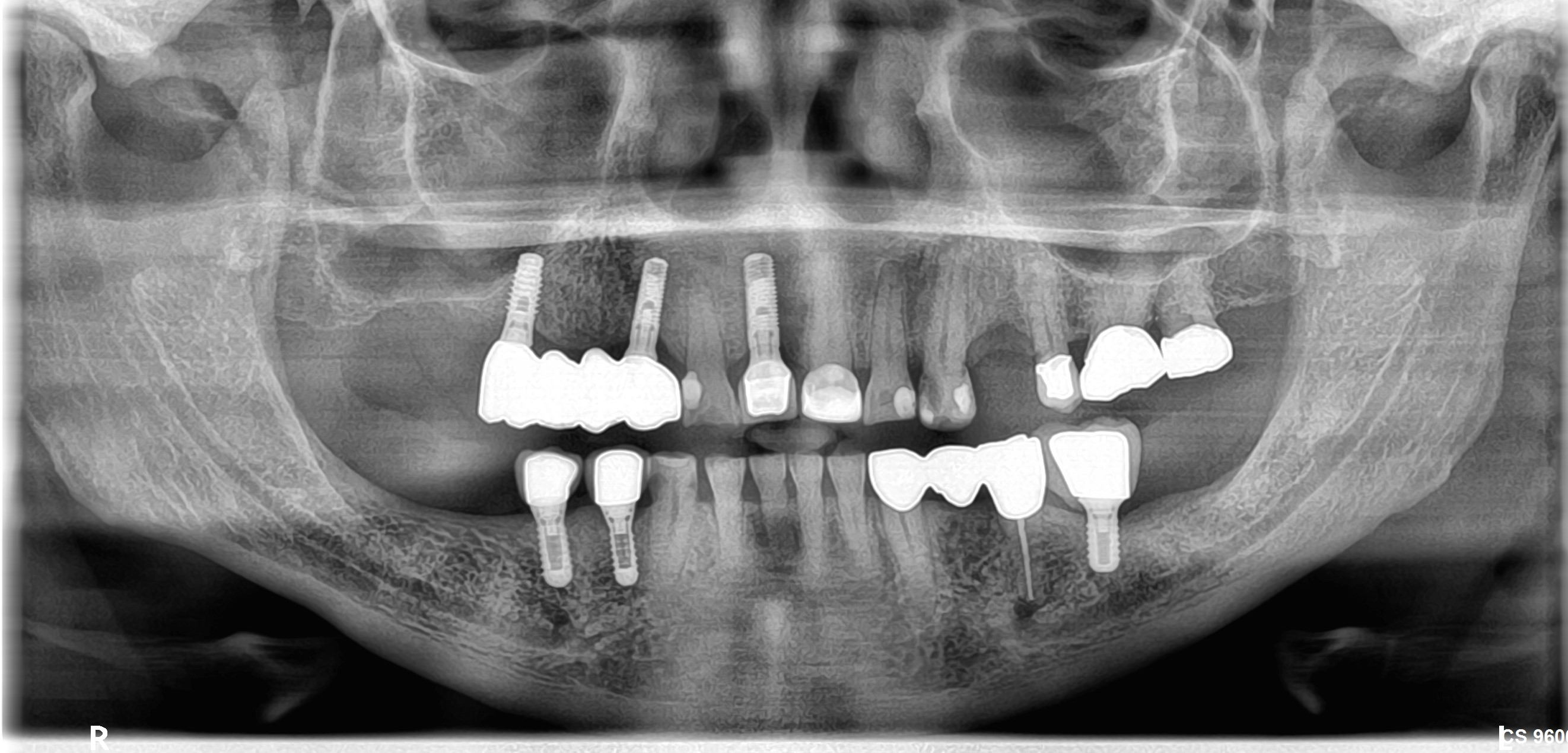
I installed 4 Intra-Lock mini dental implants last week. For 1 week post-operative, the patient said he was still feeling tingling on the lower left lip. On the day of surgery, I suspected the left side might have complications due to resistance to drilling the osteotmy sites. I decided to switch to a shorter implant for the one site near the mental nerve on the left side. The radiograph is showing the implant is about 2mm away from the mental nerve. I did not know if I should remove this implant or if the paresthesia is caused by the injection of local anesthesia being too close to the mental nerve. What do you think is causing the paresthesia? What do you think I should do?
(click to enlarge)
After Implant Placement:
22 Comments on IntraLock mini implant: what is causing paresthesia?
New comments are currently closed for this post.
CRS
2/12/2013
Is the paresthesia improving? I would suggest documenting the size of the paresthesia and follow it. It should resolve in 6 weeks, probably due to the retracting of the surgical flap or swelling. A cone beam could also show if there are any accessory nerve branches in the area, but the implants look short on the film.Could also be trauma from the local as stated. If it improves within 6 weeks I think you're good.
Leal
2/13/2013
I wouldn't worry.
When you felt the hard cortical bone you were probably starting to drill the mental foramen "ceiling".
You can see quite clearly the IAN, the mental foramen and the anterior loop and also an incisive branch, I think. You got away from those three but as CRC well said you got a big number of other chances and other small branches that can cause that small paresthesia. That happens to me once in a while. I usually draw with a red pen or pencil the areas where the pen/pencil "tingles" or "feels weird" and photograph every day or every 2 days. You will see that after 1 week and a half or two the area will be smaller.
Usually I prescribe deflazacort once a day in a variety of ways for example:
1st day 90mg
2nd day 90mg
3rd 60mg
4th 30mg
5th 30mg
6th 30mg
7th 15mg
8th 15mh
and you could go on a couple of days or stop right here.
CRS
2/13/2013
Interesting protocol, I see the patient first two weeks then a month later. I don''t prescribe anything. The nerve re- myelinates approx 1 mm per day(very rough estimate) Look at it logically you would remove or back off an implant within 6 weeks anyway, make that decision at that time. If there significant improvement then I would leave it. Full recovery can take from 3-6 months I tell patients whatever they get back in one year is what they will have. The mental nerve is pretty forgiving.
Leal
2/13/2013
I think you are deducing there is a "big" nerve damage. I am not.
Most definitely there isn't even a section damaged. And if there is it would probably be a tiny tiny branch.
Most probably there was heat and a bit of aggression to the cortical bone upwards the nerve and the deflazacort will inhibit the nerve inflammation and it would be resolved in a short time.
CRS
2/13/2013
I just have a different protocol, I give iv steroids at surgery and im steroids to prevent rebound edema . Perhaps I could be treating my own covert paresthesias! I just think that that far after surgery the inflammation is part of the healing process, but it is an interesting protocol that I will add to my bag of tricks, thanks!
Leal
2/13/2013
Sure. I am also pro-let-the-natural-inflammation-occur (but sometimes when you f.e. extract impacted canines and 3rd molars and place 6 or 8 implants with osteotomes and immediate loading... damn... if I was the patient I would want steroids). But when there is a nerve inflammation it can cause transitory paresthesia and it's better for the patient to have steroids 1-2 weeks in my opinion.
But this steroids talking can be a long multi-sided debate.
Gio
2/13/2013
Thank you very much every one. Patient is improved after the first week. At first he said it's down to the jaw now only abit of numbness on the lower left lip. I gave him Cortisone 50 mg once aday for 5 days only. should i give him more? Anyone had problem with Zorcaine injection?cause my friends said he had fews patients report of painful days after injection. I only give Zorcaine for infiltration only when i need more profoud numbness. Today is 2 weeks for him. Those are mini implants for over denture done with flapless. Patient is about 50yo and smoking. I warned him to stop for at least week but i doubt it. Dear CRS: how long after placing implant that you can remove with ease?6 weeks?hand torque?thank you very much for all your time
CRS
2/13/2013
Six weeks is a good rule to remove implants with the wrench and hand pressure. Since you we're flapless it was most likely the hematoma from injection vs flap retraction. Are you certain you did not perforate the cortical plate? I like at least a small flap to help with orientation towards the bone height. Don't know about the Zorcaine. I would suggest a medrol dose pack which loads and tapers the steroid automatically. Cortisone 50mg x five days is plenty Stop! Glad the patient is getting better so quickly.
CRS
2/13/2013
Looked up Zorcaine,I have heard of reports of paresthesia with mandibular blocks with septicaine, not sure why. My go to anesthetic is marcaine for longer anesthesia 4-6hrs ave I honestly have never had a problem with that.
Gio
2/14/2013
Thank you again everyone. I am sure not perforate the cortical plate cause i always put my fingers on both buccal and lingual side to aim for the implant. Yeah i always do flap for regular implants but not those mini implants. Patient is OK with tapping at the implants, only abit of numbness on the lower lip now. Thank you again. we just wait for another week.
greg steiner
2/13/2013
You can check the pattern of paresthesia to determine if the paresthesia is a result of damage to the mental nerve by administration of local anesthesia or if paresthesia is caused by the implant. With an instrument compare the patent's sensation of the gingiva on the alveolar crest in the area of tooth #23-24 to the gingiva on the alveolar crest in the area of # 25-26. If the nerve damage is from the injection the gingiva in the area of 23-24 will have normal sensory perception. If it is from the implant you will have paresthesia in both the lip and the gingival in the area of 23-24. If you have paresthisa of the gingiva in the area of 23-24 then it is from the implant and I would then remove the implant. If just the lip has paresthesia leave the implant. Steroids are good no matter what. Greg Steiner Steiner Laboratories
CRS
2/17/2013
I do this also to check my mandibular blocks in the attached gingiva between the canine and lateral! Great minds think alike!!!
Richard Hughes, DDS, FAAI
2/14/2013
Septocaine causes slightly more parenthesis due to the fact that it is a 4% solution.
CRS
2/14/2013
Are the paresthesias anything to be concerned about?
K. F. Chow BDS., FDSRCS
2/16/2013
Precipitating a paraesthesia with a mini dental implant is rare. The mental nerve in this case is unusually prolific and looks like an octopus. This may be the reason why the paraesthesia occurred even though the implant stayed at least 2mm away. I concur with most of the comments that it will resolve spontaneously given time. This is one of the great advantage of using minimized dental implants. Just imagine if a standard sized dental implant was used... it will probably become a more difficult anaesthesia! Using 4 minis with o-rings and housings are increasingly the treatment of choice for lower full denture stabilization due to not only affordability but also speed and safety as in this case. Recently, I noted that the Singapore Academy of Medicine has given its nod to using minimized dental implants for lower full denture stabilization. This is the first time a widely respected Asian health authority has given its official nod to minimized dental implants. I believe that it should be an increasing common sense trend in every part of the world. The full document covers every aspect of implant dentistry and is worth perusing for all implant dentists, particularly page 19. The pdf file is given at this link:
CRS
2/17/2013
I suspect it was the Septocaine since it was infiltrated in that area. The implants at any diameter would not have been in the area. If an implant is too long it will cause a paresthesia regardless of the width. Any blind technique I personally feel is a greater risk for a surgical mishap unless Ct guided with depth control. Even with a mini I without visualizing the crest you have no orientation for depth. If there is adequate width I would use a standard size implant or expand and graft. Minis are nice for provisionals. Just my opinion. Thanks for reading.
K. F. Chow BDS., FDSRCS
2/18/2013
Zorcaine and Septocaine are generics and both are actually 4% articaine with epinephrine. A Canadian study in 1993 reported 14 cases of paresthesia out of 11 million injections..... yea....11,000,000. 10 were due to articaine and 4 were due to prilocaine. So there is a infinitesimal possibility that you are correct in fingering septocaine. A CSI should look at all the clues. The more outstanding clue seems to be the crab like nebula configuration of the mental nerve which is sensory in nature. My bet is it is more likely a neuropraxia of the mental nerve due to compression as the mini dental implant is screwed in. From the OPG, it can be seen that the left most mini has strayed quite near the mental foramen due to a misjudgement of the midline. This can be avoided if the midline was defined more precisely and the minis placed accordingly. A standard sized implant is at least double the size and therefore the compression will be quadruple and more likely to cause a profound anaesthesia and not just a paraesthesia. The flapless technique is not a blind technique because we have sophisticated imaging techniques like CBCT which you have kindly pointed out. Though a simple OPG or even a primitive PA is more than enough, all of us having studied the detailed anatomy of the inter-foraminal zone of the mandible which is one of the safest places to place an implant. Even more, we have our super sophisticated thumb and forefinger that no technology to date has duplicated yet. It is not blind but virtually visualized and therefore very safe. If you go to the link in my last post, you can read for yourself in page 19 of that authoritative document co-authored by 21 of their top dentists, that two prospective studies reported 98% survival rates of minis in mandibular overdenture retention. The references are also given in the same document. Thank you for your consideration of these ramblings.
CRS
2/18/2013
It is still blind when you can't see the bone crest and you are estimating where it is. Without a cone beam I 'm afraid nutrient canals can be mistaken for a nerve. When I state that paresthesia can be caused by the local, it could have traumatized the mental nerve most likely, either from the pressure of the anesthetic or the needle traumatizing the nerve.I don't buy the compression theory and the crab nebula. And I am not impressed with minis other than retention for provisionals. However all surgeons have their preferences and I respect that, I just would not use minis when there is adequate bone in the region. I tailor the technique to the clinical situation always. I think the poster needed to be reassured that the paresthesia would resolve and was handled appropriately. We all have, myself included a tendency to preach what we feel is best based on our experience or the literature. I like to be practical and look at the clinical situation, using the available bone to best advantage with my skill set. I also like to rebuild bone that was lost. This is not meant to be a critique of the poster's work, the implants although mini, are very well placed and parallel. The paresthesia is resolving and I feel it is a good result. I just like to be able to directly see what I am doing and be sure. Thank you for your very elegant treatise and also thank you for reading. I respect your viewpoint.
Gio
2/18/2013
Thank you all again for your time. Patient is feeling normal on the gingiva of the alveolar crest between the implants-thank you Greg Steiner. He said he can eat normal only a bit of tingling still on the left lip-some time he said he forget about it. Hopefully it will be gone soon. I think we need to look at all the available for implants for patient cause not all patients had the financial to do the best option-lots of success cases for mini, short implants. Some Drs even do full mouth fix bridge with all mini implants and offered classes for it.....I mean every case is differentiated depend on patient fiance, health, age-you will not try to do extensive bone graft/tissue graft on a 80 or so right?just some thought
K. F. Chow BDS., FDSRCS
2/19/2013
Dear Gio. Healing of nerves are notoriously unpredictable. In this particular case, the chances are excellent that there will be full recovery. Also this problem can be avoided if you define the midline of the mandible precisely so that your implants will not stray too near the mental foramina. You are absolutely right that we should try our best to make dental implants affordable yet safe for every person who needs one, simply because in most cases, dental implants are the best treatment available and it is our professional and also humanitarian obligation to do so. The use of 4 minis to stabilize a lower full removable denture in the past was a matter of preference and experience because there were insufficient studies. Today it is not so. This is because there are enough studies and even prospective trials that have given adequate evidence to make the stabilization of the lower full denture with 4 minis the treatment of choice, not because it is cheaper and faster which it is, but because it is evidence based medicine. This should be welcome news for all our denture patients who currently eschew dental implants because of cost. Cheers.
Gio
2/19/2013
Dear Chow, thank you for your time. You will be happy to hear this. I had a patient tried too many lower complete dentures in the pass but she cannot wear it. she is very happy after i did 4 mini implants which stabilized her denture right away in an hour. Now she wants to do the top for her. Too many cases like this, or like short implants..Thanks
K. F. Chow BDS., FDSRCS
2/20/2013
Gio, that is really wonderful for your patient and also most satisfying for you as a professional. And it did not cost an arm and a leg, just 4 affordable minis and an hour or so plus minimal trauma. We should replicate this experience for many many more of our elders.The loose lower full denture has been a bane to patients and dentists alike. It is an increasing problem because of rapidly aging populations throughout the world. The world will reach aged status about 2040. Aged nation status in UNspeak means 15% of the population having reached 60+. About 30% of these aged are edentulous, which means that many of our elders are suffering from malnutrition, poor self-esteem and low quality of life, all because they cannot eat, speak and socialize due to loose lower dentures. We dentists actually now have the means to ace this problem with mini dental implants! Nuff said.