Thoughts on slightly angulated implant?
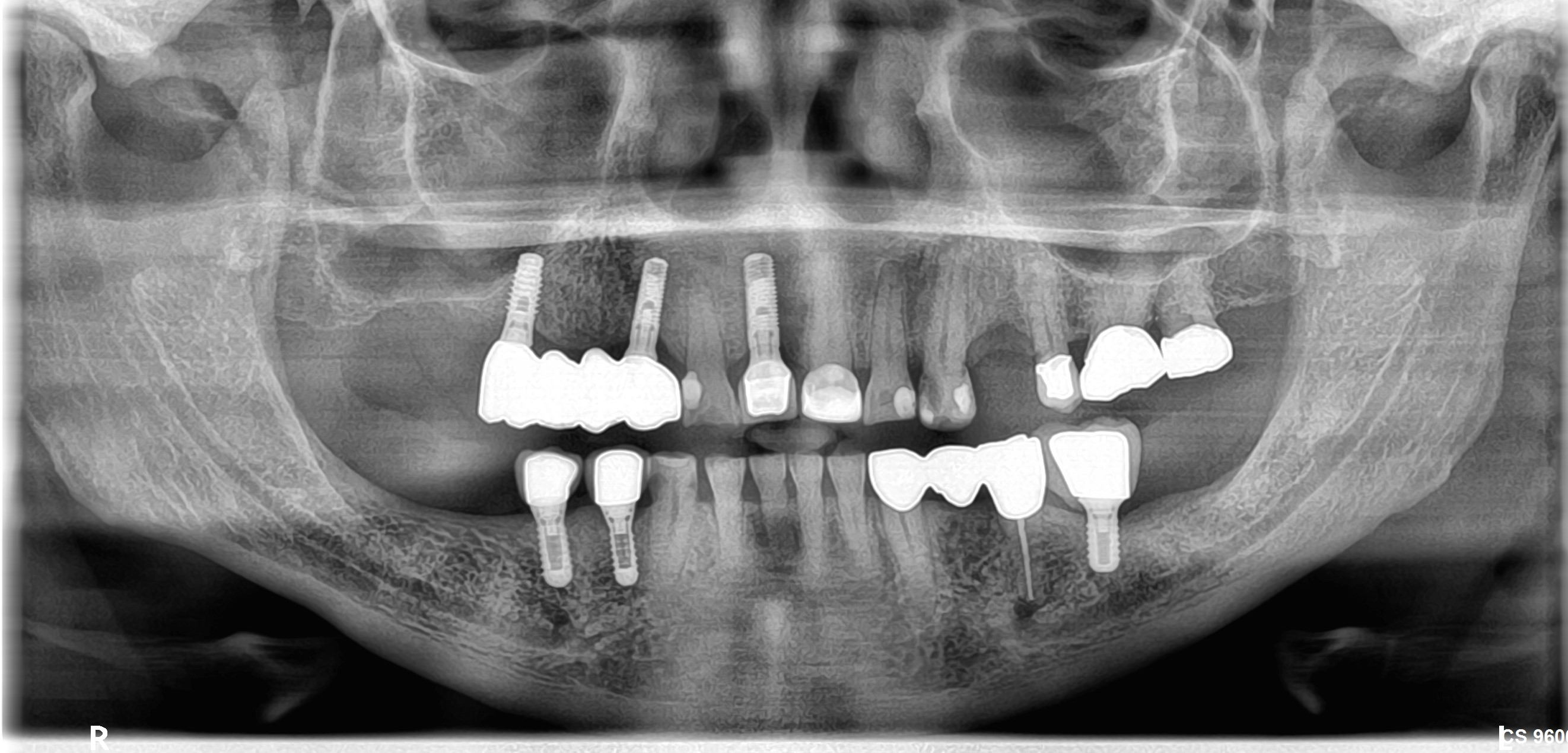
I installed an implant in #30 site [mandibular right first molar; 46] using CBCT and a surgical guide stent, but still found end result to be angulated. While drilling the osteotomy, the drill was deflected to the mesial because of an area of dense sclerosing osteitis (this was know on pre-op preparation but unknown that it would force me mesial). After surgery and upon seeing the angulation I tried in the surgical guide again and noted that the centre of the healing abutment was about 2.5 mm distal to the ideal center of the final restoration. The orientation in the buccal- lingual dimension was right on. Because of this only 2-3 mm discrepancy from ideal, the implant was left as is and the patient was informed of a slight variation from ideal and it was explained that the presence of the dense bone island would make ideal placement more difficult. I realize the implant restoration will be bulky on the mesial aspect and not ideal but I believe the restoration to be functionally good and this slight deficit outweighs removing the implant and repositioning which would compromise otherwise healthy bone with a larger osteotomy. What are your thoughts ?
![]IMG_1649](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2015/04/IMG_1649-e1429496061837.jpg)















{kind=link}
{kind=link}