I recently posted a case of a failed All-on-X and it appears that it was taken out of context and offended some. The attached photos are of a case I am currently working up with a restorative doc and a lab technician. As part of my evaluation, I always do a face bow transfer and mount on an articulator (not always a pretty mounting but mounted). This allows me, as the surgical member of the team with a fair amount of restorative training, to evaluate the patient vertical and begin the conversation with the team about how to go about creating the necessary space. Yes, I do CBCT and everything else but to me, this is the critical step and I have seen enough problematic cases with concave intaglio on the prosthesis which is clear evidence of inadequate space. My intent when I posted the last case was to stimulate a conversation about treatment planning but apparently, my wording, or perhaps that I identified as a periodontist, was offensive so here is possibly a better way to stimulate such a conversation.


David Lerner DDS comments:
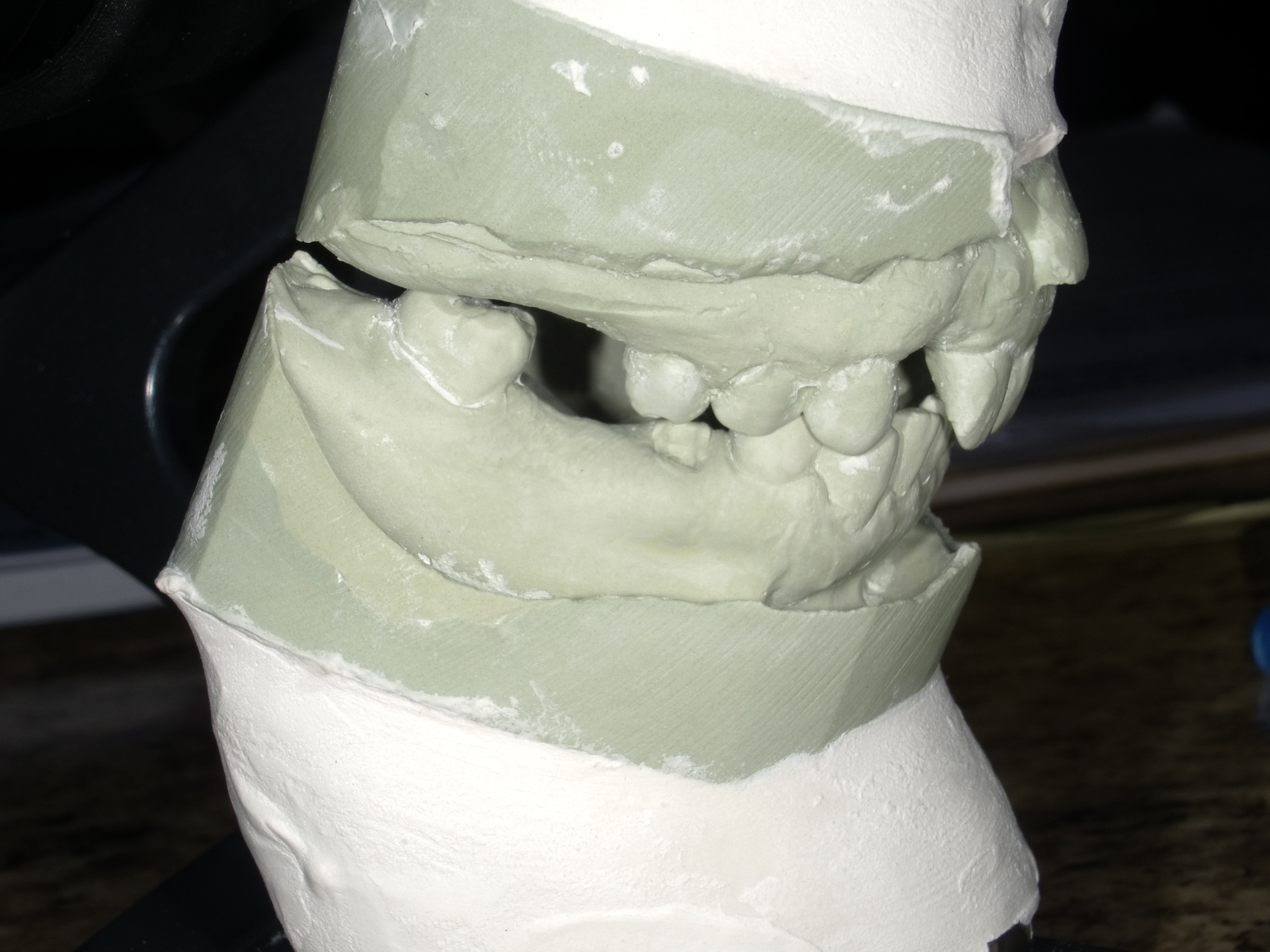
It appears that this case is collapsed and overclosed with the mandible retruded. An evaluation should be done of TMJ and neuromuscular physiology to determine proper jaw relationship before development of a surgical and restorative plan.prosdoc comments:
What are these casts for? Partially edentulous reconstruction? Full arch dentate? Full arch implants? Each tentative treatment plan requires different cast designs (border molded etc) and mountings (hand articulated, CR mounting, etc). Also, a change in vertical dimension is not diagnosed on casts, it's a clinical diagnosis which is then transferred to the casts. Many times the teeth supraerupt over time, maintaining a physiologic vertical dimension. I decide clinically if the VDO needs opening then make a CR record at the ideal vertical with the joints in CR (CO for us pros nerds, i.e. tooth position when the joints are in CR). Then when the casts are mounted with the pin at "0" I know how much interocclusal space I have initially and can begin the restorative diagnosis and treatment planning along with determining bone reduction/addition and implant positions. So simply mounting casts (you didn't mention if you hand articulated these or had an interocclusal record) doesn't give us that much additional information.Carl Crutchfield comments:
CRO 😉Timothy Carter comments:
But it begins a treatment planning conversation. The average doc I work with does not have your prosth knowledge and by my last survey only 3 of my referring docs have an articulator in their office. I have chosen to educate myself and take additional records for the simple reason of getting the team involved and thinking about a plan... so I will have to disagree with your statement that these provide very little information. Yes this is a simple mounting in CR using the Dawson method and by no means represents a final solution... but it starts a conversation. Hopefully by doing a few simple things in the beginning we can avoid the common critical error of attempting to restore with inadequate restorative space... that will lead to concave and rough intaglio surfaces with filthy ridge laps!! Simple but effective! I Hope!!!Joe Nolan comments:
Surely there are many people out there with concave ridges in various levels of concave, who have been ignored by both specialist and general dentist docs doing the surgery? The altar of expediency and let the patient power hose mentality...ST comments:
In my humble opinion, unfortunately, what is usually missed from these elaborate full mouth reconstructions is the initial malocclulsion, which is probably why the patient has ended up in this state. Even from these simple casts that provide very little information, it is clearly evident that the arches are very narrow and the mandible is retrognathic, resulting in a deep, traumatic occlusion. The significance of this is that no matter how well this case is planned, the final prosthesis will eventually have the same fate as the patient's original dentition unless 1) they are very old to outlive it 2) the restoration is made in acrylic so it compensates the occlusal forces and it "gives in" making it easy to repair 3) the patient has a very soft diet and does not brux. If the initial malocclusion is not resolved, any prosthetic plan is destined to fail at some point.Bruce Smoler DDS comments:
I appreciate your candor and your desire to not step on anyone's toes... a refreshing respite at times from the occasional Big Dawg mentality circling the Full Arch Implant realm some of us cohabitateJigsaw comments:
Mounted casts are great. Photos are also very important. Evaluation of the transition line. Alveoloplasty. Surgical placement. The list goes on. Bruxism. This work is not for the weak🙏🏿🙏🏿🙏🏿🙏🏿