I want to place an implant after extraction of this 76 tooth. But, I'm concerned about the lesion underneath? Thoughts on this? Can we place an implant?
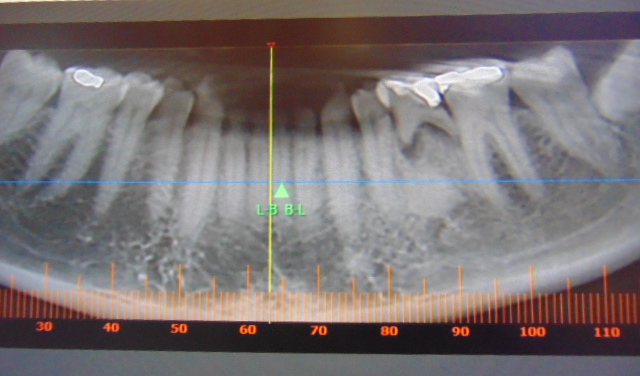
I want to place an implant after extraction of this 76 tooth. But, I'm concerned about the lesion underneath? Thoughts on this? Can we place an implant?
Neil Zachs comments:
Personally, I would be concerned as well mainly because as you know, vascularity, or lack thereof really affects how an implant integrates. Maybe take it slow and don’t do this as an immediate case. Debride the site really well of any and all infectious tissue and assess how well the site bleeds. Maybe even take a bur and hit the area a few times to decorticate and see again assess bleeding. These lesions are REALLY areas super dense and tend to be really Avascular. Move with caution to avoid failureRichard C. Adams comments:
I would agree interns of presiding slow and determining the vascularity of radiopacity in questionMark Adams comments:
Dont worry there is only solid bone here so just tap it out like you would in D1 boneAnonymous Anonymous comments:
Doesn’t look like an odontoma. More likely Idiopathic osteosclerosis. Like Neil said very avascular. However what are our options? Deciduous tooth needs extraction and curettage of socket with graft. Other then implant your not cutting down the adjacent teeth for a bridge. However the avascular bone does warrant waiting a little bit longer. Use copious amounts of cold water irrigation. Antibiotics pre and post op. Don’t be afraid to torque down more then usual, studies have shown that higher torque does not induce necrosis in dense cortical bone.Tim comments:
I would not be concerned about pathology but, like others have said, lack of vascularity. Unlike Neil though I would do it as an immediate that way if it doesn’t work you can move on to the next option a little sooner. IMHO waiting is not going to change the vascular makeup of the site so may as well complete it in a single visit.Dennis FlanaganDDSMSc comments:
Remove the tooth and biopsy the bone. You don’t know at this point what that isGuest comments:
Several options - Send your scan to an OMFR for interpretation . Take a biopsy with a trephine at extraction if you are worried and have it analysed or refer to OMS and be content with the abutment and crown restoration.guest comments:
I would do it guided, trephine out most of the lesion, place a PRGF graft and wait a bit, see that type of healing you get, say 12 weeks then place the implant letting patient know the prognosis is guarded. Wonder if the sclerosis is related to the infected primary.Greg Kammeyer, DDS, MS, D comments:
I agree: biopsy will confirm diagnosis and increase vascularity for the implant laterRichard waghalter, DDS comments:
This condensing osteitis is in a walling off response to the periapical lesion from the mesial root infection from the over retained deciduous tooth. The patient is obviously over the age of 18. I recommend extraction of the baby tooth and replace with free-standing dental implant. As precaution one might consider prescribing Amoxicillin beginning the morning of the extraction. The condensed bone is type D-1 and is excellent for long-term prognosis for implantation. Caution in restoration means to be sure there is immediate cuspid rise excursion in CO and CR. Traumatic occlusion is probably the most detrimental insult that destroys dental implants.