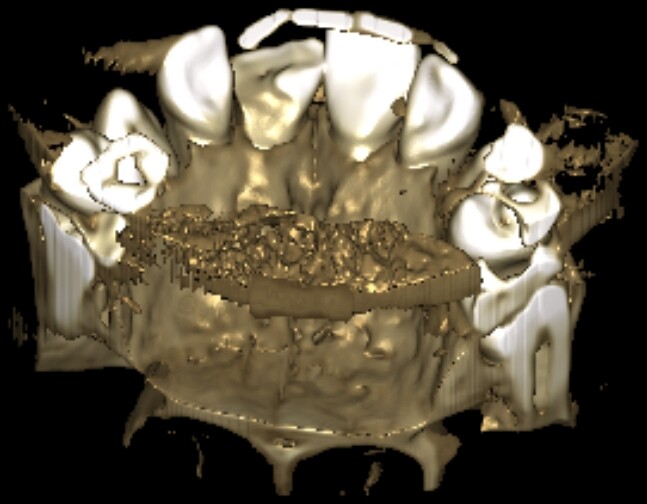
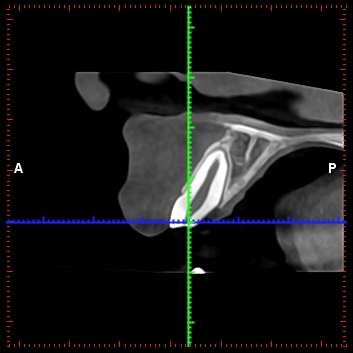
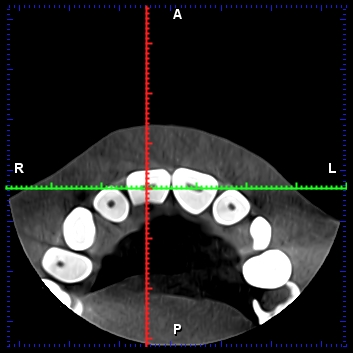
Hello colleagues. This is a patient, an 11-year-old boy, who fractured tooth 11 (European classification) while playing . The child visited the office 7 days after the incident. Tooth 11 is still vital, but with an open pulp chamber and reduced vitality. The tooth has a 2nd degree of mobility. In addition to the large fracture of the crown, there is a second oblique fracture on the palatal side, which reaches the bony edge. Please guide me for the right approach to treatment!
Dr b comments:
Root canal, post, composite buildup of crown. Long term px.poor but should get many years out of it
Matt Helm DDS comments:
Long term px guarded only momentarily, but quite favorable in the future. Managed properly and conservatively (a post is out for now) this tooth can provide a few decades of service.
james singer comments:
as per dr b, and maybe consider ortho extrusion
Matt Helm DDS comments:
Much too early for ortho extrusion.
Perrydon comments:
I agree with first response, however if the tooth cannot be restored without crown lengthening it should be extracted and replaced with a Maryland bridge until the appropriate age for an implant.
Matt Helm DDS comments:
Examine everything you've said to find out how wrong you are! You said "if the tooth cannot be restored without crown lengthening it should be extracted". Read that again! I don't know in what proper dental treatment world it makes any sense to extract a tooth like this one, with plenty healthy hard structure remaining, simply because you can't do a crown lengthening! And who said that a crown lengthening is even needed at this time? Be more careful of your "advice", because what you just advocated is plain butchery in my book. I strongly advise you to get more training. Not trying to be mean at all here, but if we're going to teach on this forum, we may as well teach the right things, or not teach at all and keep quiet when we are outside our area of expertise. Sorry, but your statement was so wrong, so over the top that, with all due respect, it needed to be addressed!
Matt Helm DDS comments:
A post at this time (specially a cast post), carries too great a risk of root fracture resulting in the irreversible compromise and premature loss of this tooth! Crown is also excessive and unwarranted over-treatment right now. It's too early for tx that is invasive and destructive of sound tooth structure. It risks early compromise of a tooth that does have a promising prognosis if managed conservatively.
Matt Helm DDS comments:
WRONG! It's much too early for post crown! Conservative is the KEY here. Remember the AGE of the patient! Don't go plowing ahead with your head forward when you haven't even "looked around" yet!
Charles Brent Geffen comments:
I’d try and avoid the post ( pulpal chamber can support a good core). He’s probably a boisterous active guy and future trauma may result in root fracture and thin buccal plate destruction which will definitely require more extensive future treatment. His hygiene is appalling and regardless of this phase of treatment all will fail if he isn’t compliant and continues to be so neglectful : a little bit of education will go a long way in solving this easily without surgery.
Dr J B comments:
Poor oral hygiene needs to be addressed. Is your question whether an implant should be considered? ( this is predominately an implant forum). If it is, I think the answer is no. If there is any way you can restore the tooth you should try that, whether it be a direct pulp cap ( although its a little late for that), or root canal post and crown, or laser gingivectomy and bonding. The fracture on the palatal looks concerning. Implant possible only after skeletal growth completed.. Could also consider a cantilevered pontic if tooth is ultimately lost, use tooth 21(your system). The pontic hangs off a laminate, great long term temporary. Can remove with laser and reuse if you're lucky if need be. I've seen research showing cantilevered (only supported on 1 abut)hold up better than Maryland(supported at 2 ends). I use a Cerec to design and mill inoffice works great. Good luck.
Peter Hunt comments:
Your commentators so far seem to want to preserve the tooth with conventional therapy. I agree with this approach for one main reason, an implant placed at this time and to this gingival level will at the age of 20 be 1-2mm more apical because the adjacent teeth will have continued to erupt. It's always a good idea to defer implant therapy until they are more mature and have finished growing.
Matt Helm DDS comments:
How much do you want to bet that properly and conservatively managed it will be decades before this tooth will require replacement with an implant? You're talking over-treatment before the real treatment has even started.