I am entertaining suggestions for replacement of this bar. I inherited this from a deceased oral maxillofacial surgeon. Evidently he created the bar out in Oklahoma somewhere. I’ve never seen extensions on a bar case like this and have never seen a town as crowded. She is miserable. I would like to know of your suggestions. I’ve made cocoons for the upper and lower Appliance. I had to block the bar out with boxing wax. Once I take the bar off I’m putting healing colors until I can design something that is suitable. Requesting your input. Thank you so much for your professional input. Dr Bill Woods.


Dr T comments:
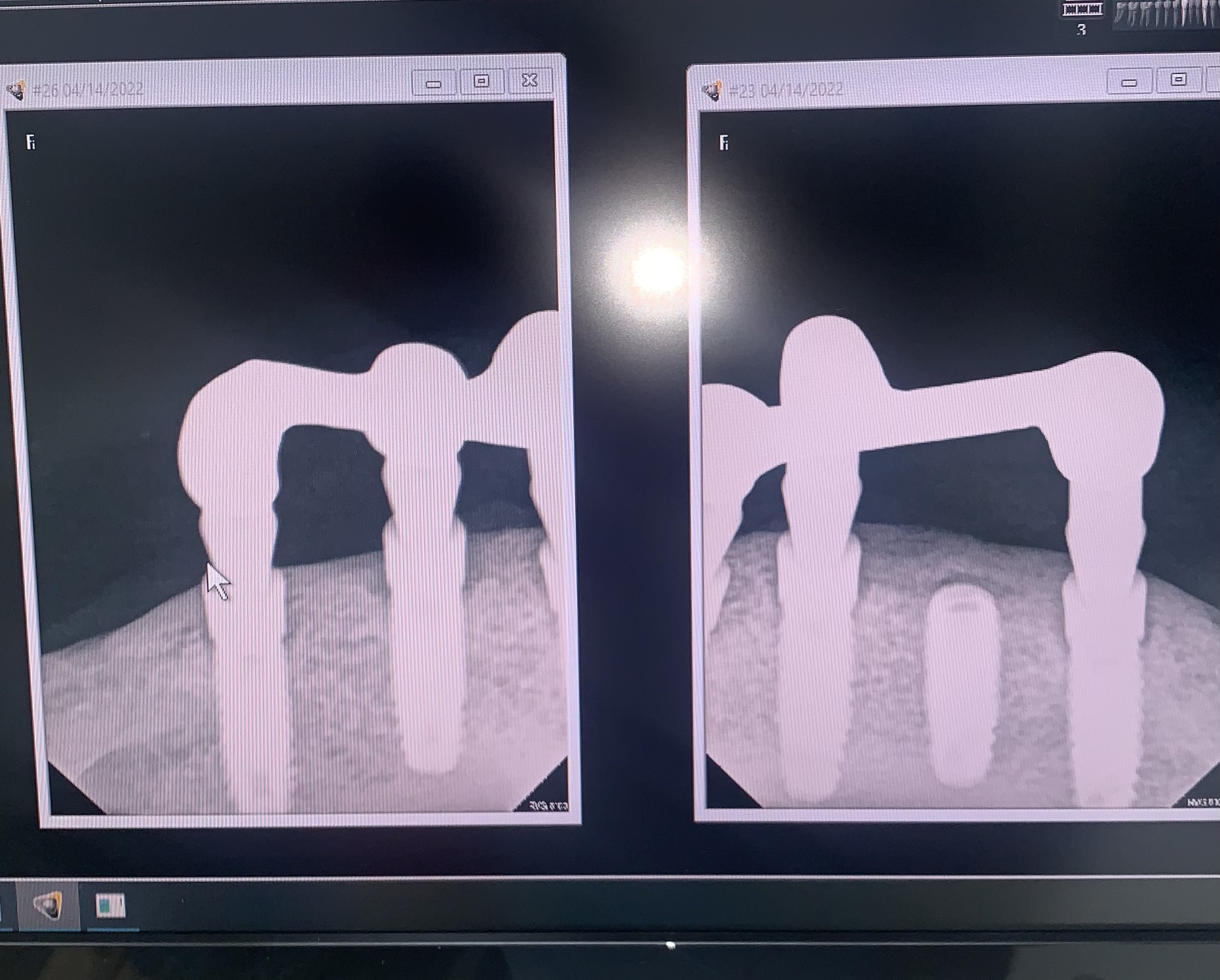
The bone around the fixtures looks great!! Why is this patient "miserable"??Dr. Dobs comments:
Agree with Dr. T. Why is she miserable? Is the upper denture unstable? Does the lower bar not provide the retention that would be ideal? Is she xerostomic and have issues with lack of intraoral moisture? The pictures show excellent oral hygiene around the abutments and the radiographs show excellent bone levels. Is there an occlusal relation issue. Please advise and we can all offer some suggestions.Bill Woods comments:
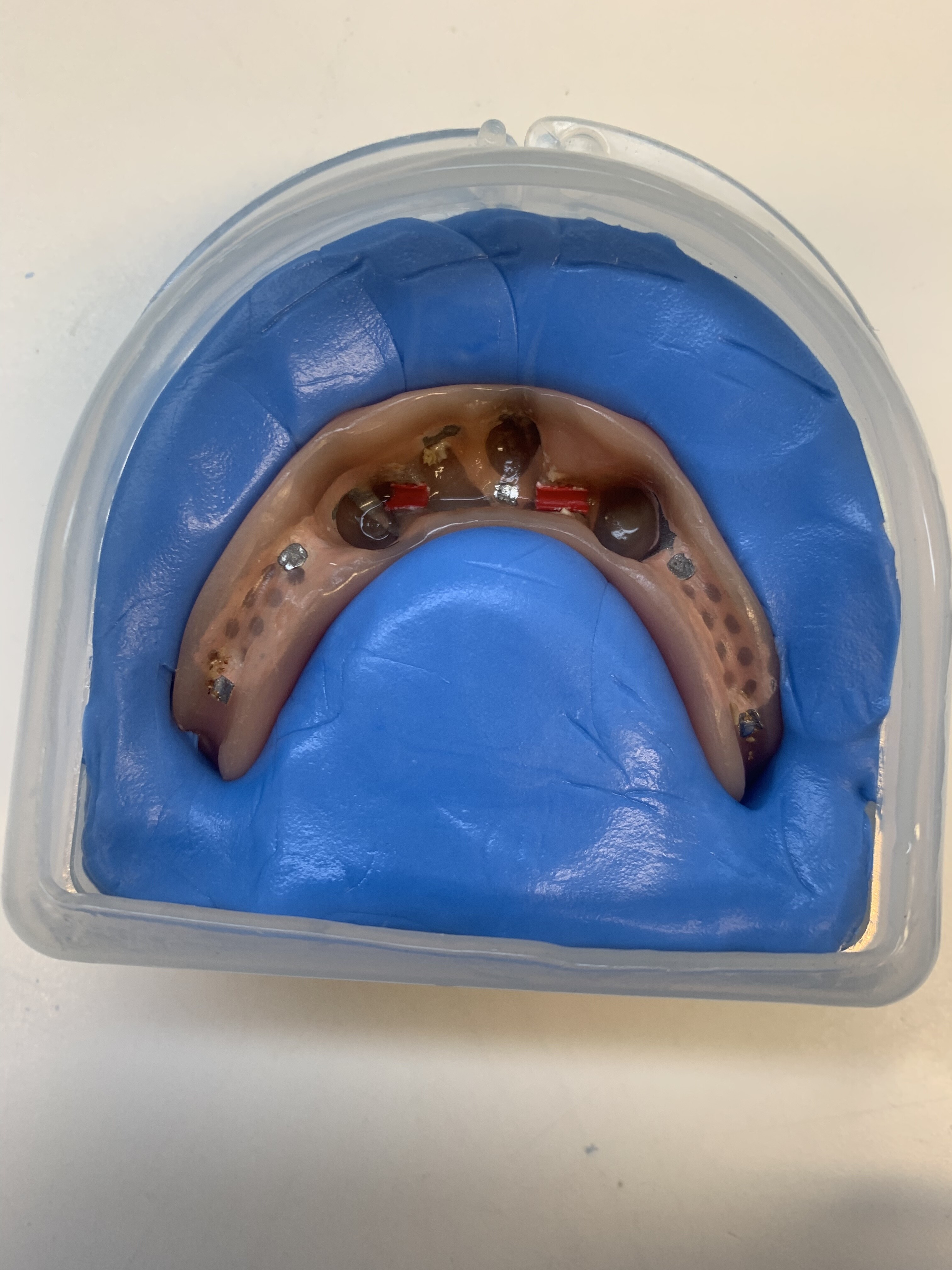
The bar severely crowds her tongue and has been a comfort issue since she received it. She has always hated it, and often has lingual frenulum issues. Too much prosthetic hardware in the midline lingually. I can improve that. Esthetics I can do that as well. Redesigning prosthetics from point A>B was my interest. There have been great suggestions. I’m very grateful! Thank you.Gregori Kurtzman comments:
I see one implant fractured crestally and is not in the current bar, I would ignore that one. I think the current bar it too tall and in remaking it I would lower it closer to the tissue and also have some curve to it following the arch curve. I would also cantilever a Locator attachment bilaterally and place 2 others in the anterior area ( to the left and right of the midline implant. Take a bite with the current denture in. Best way to start this is take an open tray impression after the current bar is removed. Replicate the current denture to get the VDO, while the bar is out fill the tissue side of the replica denture with a medium VPS and insert and articulate into the previous interarch bite and have the pt occlude. Reinsert the old bar and dismiss the pt. Send the replica lower that was relined, the open tray impression and the upper arch impression to the lab to have the new bar made. lab will return the new bar to try in and a waxup over that of the new overdenture. Try in the bar make sure it seats passively. Radiographs to confirm full seating. Try in the wax up verify the VDO and esthetics. Reinsert the old bar and send to lab to finish the dentureTim Carter comments:
The first question would be directed towards the patient and I would ask “what do you desire”? Then it is an issue of finances and the restorative docs level of comfort with different restorative options. It looks like the upper arch is edentulous so 4-5 implants is potentially overkill. You could use only 2 of the fixtures and place Locators or you could have a new more traditional bar fabricated. Interocclusal space doesn’t appear to be an issue so multi-unit abutments and a fixed hybrid is a potential option.Bill Woods comments:
Finances aren’t an issue. Plan to improve esthetics and get that chassis out of her mouth, realizing that I own it once I proceed because I’m certain I could never get that assembly back together again!Dennis FlanaganDDSMSc comments:
Is there an osseous crack near the symphysis? Better get CBCTBill Woods comments:
Dennis, I saw that early on but thought that the Cat scatter might be a factor but you are correct. That is something to rule out. Thank you. ( not related but Incidentally about 16 years or so ago I posted a difficult maxillary anterior case on a 17 year old and your first question was how many had I done!! Great point. She left only to get it out and get a partial at another office!! Whew!) thank you for your professional advice over the years. I haven’t been here lately but plan to return! BillDr K Gilani comments:
Upper jaw likely to be too atrophied for implants. Just replace the lower bar with a modern milled fixed restoration with good aesthetics and you are a hero.on the top a full denture of course.Prostho Wolves comments:
If you have the implant connection information then contact C+M (Cendres & Meteaux) and review the SFI Bar protocol. It's rapid, chairside and you can control the vertical hiegth of the bar to some degree if you have occlusion issuesKent Mueller, DDS comments:
there is a lot of hardware in situ to provide passive retention, at worst ; hygiene in function may be a concern for patient. Occlusion wear patterns appear minimal. Perhaps prosthetic cosmetic issues and VDO may be an a contributing factor with regard to patient dissatisfaction. ; Speech may also be compromised by lingual placement of retentive hardware .I am not impressed by Hader clip retention hardware; perhaps this patient is not either.
I like Dr. Tim’s consideration of individual ‘ball’ or ‘locator’ attachments with a lower profile on 3 implants. This gets you at least to an affordable transitional set-up as a trial + this may better obturate existing mid-line open lingual flange area.
Bill Woods comments:
My plan exactly. I already have locators present. Do you agree these are Zimmers?Tim Carter comments:
At first glance I would assume Zimmer but the “Vent” hole at the apex is more round than the Zimmer which is oval. The thread pitch is more aggressive than Zimmer and the taper doesn’t match. Possibly a clone but it appears that the attached prosthesis is that of some other brand as well. I am an avid Zimmer TSV guy and they just don’t match.Adil Albaghdadi comments:
I did not understand what's the chief complain and the diagnosis? How old is the Patient? why not consider a fixed VS removable since the arch is small U shape and AP spread may allow to add one molar each side if the patient wants a comfortable prosthesis? Fixed against removable has little occlusal force on implants plus you provide a good comfortable solution to the patient. Good luck with you case.sb oms comments:
what a mouthful, the bar impinges the tongue. This would drive me nuts. This is a no brainer, fixed hybrid to first molars, not much A-P spread but it will work against an upper denture. You can place shorter multi-unit abutments to create more space.Dr Bill McFatter comments:
I don't know if you have enough AP spread to do fixed - this bar appears to have been design with 0 movement in that the posterior screw platforms won't allow compression and with any loss of tissue support you have the potential for cracking the prosth or torquing the implants You will need to create some movement/forgiveness in your design if you are going to repeat a RP-4 design as was this case- you will depend on tissue support and this will change over time as the posterior ridge continues to resorb so you build in protection you might consider a lower profile bar with distal ball abutments ( these will allow compression- (a class 5 movement potential in function) since your function will be mostly distal to the most posterior implant and an anterior hadar clip- The Hadar clip will give you an early warning when you have lost soft tissue support because the prosth will start coming loose in function - you will want 3 month recall to check ball abutments ,hadar clip and posterior loss of support (possible relining this area-be careful to watch changes in the occlusion Keep the occlusion from bi back and be sure there is no anterior contact in function Once the functional dynamics start to change you will start to see anterior occlusion show up you will need to eliminate this by trying the above things first Bill McFatterOleg Amayev comments:
I hate these bars. So much metal in the patient mouth. Just place locators and get it done.