I just did a case today. 2 extractions(1.5 and 1.7), a cystectomy in area of 1.7. I placed 2 implants in position of 1.4 and 1.6 (with sinus lift lateral approach). Clinically, I measured the distance implant-teeth, implant -implant. The distance between implant 1.4 and 1.3 was more then 2.3 mm (I tried to place it more to the alveolar of 1.5 ). After 2 Rx it shows that it is in contact with 1.3. (I know that to be sure I need to do a CBCT).Can you give me an honest opinion, and advice on this case? Thanks in advance.


M.K. comments:
You're correct that a CBCT would have been a good way to determine the 3D position of the the 1.4 implant in relationship to tooth 1.3.But a series of PAX’s at different angles might show that there is separation between the implant and the root of the natural tooth.
If you’re unsure, then you may want to consider contacting the patient very soon and remove implant 1.4, socket graft and place another implant in 4-6 months. If you’re thinking of going route, do so before the implant and bone start integrating…I think you have about a week from the time that the implant was placed (I’m sure others would know more precisely than me).
Is the patient experiencing any discomfort from tooth 1.3 while functioning?
By the way…the sinus grafting of 1.6 looks really good…just asking and not a criticism…but would a sinus graft through the osteotomy of 1.6 have been another alternative?.. it looks like there is sufficient vertical volume of bone below the sinus floor to stabilize the implant from an osteotomy technique.
aminmo66@yahoo.com comments:
I don't think OPT is a good way to judge distance between 13 and 14. You can see a lot of overlap between natural teeth too. Take periapical radiograph and you may find that your implant positioning is spot on.Faisal comments:
Don’t do nothing. If you touch the implant and disturb the healing cascade the implants a goner. I’m sure clinically when you see it in the mouth it should have enough space to receive a reasonable restoration. If the implant survives the first 2 weeks it’s in the green. If that happens wait another 6 weeks and root treat the canine if it’s symptomatic or showing radiographic changes. Good thing is that it’s already got a crown on it, so it’s already prepped underneath. So again if there is no pain in either tooth or implant: don’t do nothing!John T comments:
Look at the roots of 2.3 and 2.4. They appear to be overlapping but you know they can’t be. I agree with the other contributors that an OPT is unreliable, particularly in this area of the dental arch. No need for the expense of a CBCT, just take a LCPA view of the canine-first premolar interspace.Tim comments:
I agree that it is just overlap from the PAN. What bothers me about this case is that you have enough confidence in your ability to carry out all of this treatment but lack confidence in your diagnostic skills and thus propose such a question.Oanca Alexandru comments:
i am passing a period of fails,so i kinda lost my courage.I found about this forum ,read ,and saw some smart answers from great Dr.(not just critiques).I am not ashamed of my stupidity some times,i want to progress.Matt Helm DDS comments:
The other contributors are right about the radiographic overlap of the implant in the 14 position and tooth nr 13 (the canine). That overlap is plainly evident on both panoramics. And yes, it is very possible that if you take a pariapical x-ray with the beam perfectly perpendicular to the tooth-implant space you may discover that the implant doesn't actually touch the root of the 13. That said, however, it's still a moot point (that is, it's purely theoretical), because the nr 14 implant is still way too close to the 13, where it shouldn't be. Perioperry is the only one who truly hits the nail on the head by addressing the real problem, i.e. the evident impossibility of having a proper gingival embreasure and creating a proper interdental papilla. The absence of a proper papilla and embreasue WILL BE an aesthetic problem in that area, and one that could esthetically compromise your case. Did you ask yourself why you're coming out of a period of fails? Is it possible that you rush a bit sometimes? I'm not trying to be critical (you did a great job on the sinus lift) but there really was no reason for the 14 implant to end up so close to the 13. Another millimeter more distal would have been ideal. Now, I KNOW that you are Romanian. Your name and your English mistakes are the dead give-away. :)) (BTW, "Rx" in English means "prescription", not x-ray as it does in Romanian. The proper English term for a periapical x-ray is "PA", and for a panoramic it is "pan".) I know pretty well how dentistry is practiced in Romania. You just "bumped" into an American-Romanian, LOL. Are you practicing in Bucharest? With my decades of experience in New York, I could teach you a lot. If you would like, I can give you my e-mail and you can write me. But I will only do so if you specifically ask for it and agree to correspond one on one. I wouldn't want to open myself up to accusations of impropriety. Astept asadar raspunsul tau. :)Matt Helm DDS comments:
One more thing, if I may: NEVER lose your courage. It is evident that you are a good Dr and that you do pay attention to the important details. The simple fact that you are open to other opinions shows that you strive to be your best. Keep it up and don't allow yourself to get demoralized by little imperfections. Little misshaps will happen, sometimes even with the best of intentions and efforts! Such is the nature of our profession. You're doing just FINE!Oanca Alexandru comments:
Hei Dr.Matt yes , i am romanian but i don’t practice in Romania,currently i am working in Norway.Teoretical staff from what i now is that u need to have a min of 1.5 bone between tooth ,implant ,that can sustain a healthy papilla.I was aware of this measured clinical and the bone was more then 2:(.My only upset is that i should have given a better angulation more parallel to the root of 1.3:(.Its a very good thing that you want to help me and i appreciate that.It would be nice to have some down to earth Dr. with who can i corespondMatt Helm DDS comments:
If you're in Norway (brrr, too cold for me there, LOL) you have an advantage that Dentists in Romania don't have: you have access to all kinds of implant courses all over the world. Do yourself a favor and use it. (Well, at least after this stupid pandemic dies down a bit more.) The pearls we learn along the way in this profession -- far removed from the dental school classroom -- are mostly "stolen", copied, from others who have gone before us and have much more experience. While I certainly understand why you wanted to have ideal distance from the 14 implant to the 13 root, in my view, with all the space you had available, you could have easily gone 0.5 mm more distal with the implant -- indeed, you should have -- and been safer, if we're going to nitpick. And nitpick we shall, because the devil is always in the details in Dentistry. :)) Even if the head of the implant had ultimately ended up 0.5 mm too distal, it would've been easy to compensate for it in the final restoration by simply adding a little more porcelain to the mesial contact area of the 14, but at least that way you would've been ensured a healthy-sized inter-dental papilla -- important in this area from a cosmetic standpoint. Also, trying to angle the implant to be parallel to the 13 root is not an easy feat, unless you possess either truly superior visual space orientation skills (and use the labial canine bony convexity as a visual guide), OR if you have a surgical guide. I always feel that in cases such as this, pre-operative prostetic planing and a model wax-up are imperative for ideal results. Here is a suggestion, and you can write me about it at dasmileman (at) yahoo (dot) com. The old-fasioned way to prostetically pre-plan your implants in a case like this, before the age of computer-generated surgical guides, is to fabricate a clear omni-vac stencil (gutiera transparenta) over the model wax-up, which you can then use in the mouth during surgery to better orientate yourself. Perhaps in other cases it's not so crucial, but in a case like this which involves the anterior aesthetic area I feel it's a must.Oanca Alexandru comments:
Thanks for you time .Yes i am going to courses ,but this first premolar is like my weak point,i feel bad when i place a not straight implant(even tho i do 4 or 6 implants with last 2 tilted)Even if i study cbct and have in head the position of the root,canine...(but in this case i saw on cbct that was pretty straight).I will take first some X ray ,and if not Cbct.I feel bad taking out the implant but i need to do what i have to.Oanca Alexandru comments:
Thanks for answers.The implants were placed today.I saw that the root of canine is slightly bend to distal,thats why i prepares the osteotomie more to the alveola of 1.5 and in a more palatal position.I measure the distance from the neck of the 3.5 implant to the root it was more then 2 mm.When i insert implant i made so that is angulated as the root of canine,not in a straigth path.Maybe because i placed it not in center of the bone but little bit palatal its seem like the body of implant is on canine?My concern is the apex?Thanks for help guysPerioperry comments:
The response by MK is good. Also, the implant and the canine tooth may survive just fine, but one thing that is of concern is the restoration that will be supported by the premolar. How can an embrasure sufficient for interproximal tissue health and plaque control be developed when the implant is so close to the canine? This worrisome result could likely have been avoided by preoperative evaluation & planning to produce an intraoral surgical guide. A CBCT and implant software, and/or a diagnostic wax up should be routine in cases such as this one.Oanca Alexandru comments:
Clinical,the implant is distal to the normal place of 1.4.I remember that i checked with paro probe to aee distance from 1.3 and it was more then 2.Clinical bone it was to suport papilaa:(ORAL SURGEON comments:
They look good to me.Dr Zoobi comments:
The mandibular teeth are overlapping on the panorex the same way your implant. You can not judge implant position from a panorex. Take a periapical radiograph to verify proximity to canine. Cone beam would be preferable. Nice work btw. Some cases fail. The objective should always be to learn why each case failed and grow from it. It’s the process of being a “seasoned Implantologist.” Always give it your best and learn. Keep learning. If you hit a rough patch, lay off for a bit and get extra training. Find mentors who love to discuss this stuff. You can email me anytime if you have questions. drzoobi@gmail.comdrbagur comments:
Dear Alexandru... You worked hard. At this juncture,CBCT is better for your peace of mind. Opinion wise- TP looks like given more surgical importance than restorative approach. I had similar case- placing implant in upper first pre-molar area crossing vital canine [Pre-CBCT era], kept canine under observation for over 5 years. Canine survived. Similar cases you could could think of Basal-Cortical implants. Best Wishes. Dr Bagur BDS MDS FDSRCS Ed. Oral SurgeonRamin comments:
I am greeing with Faisal Be calm and wait. It happened to me and after several years every thing is safe and sound The one and only problem is tittle tattle of naughty dentists in future that will judge your practice in front of your patient To show themselves as the best even if your patient be happy about implantsOanca Alexandru comments:
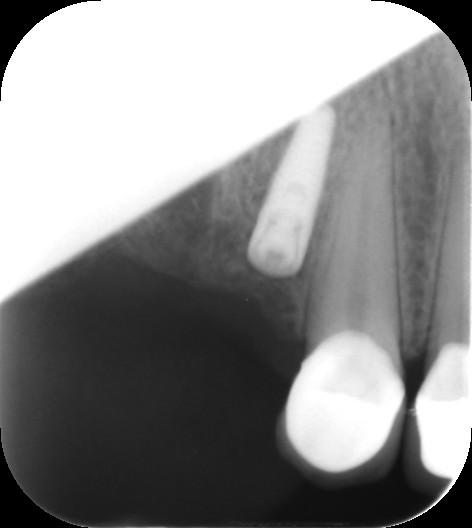Update of the case…I took an Rx (not the best ,i am not that good ,and never was to interested in becoming better on taking Rx,maybe i should).Pacient is asimptomatic,no pain,pressure on 1.3.Maybe i should take a CBCT when she comes to remove stiches?.