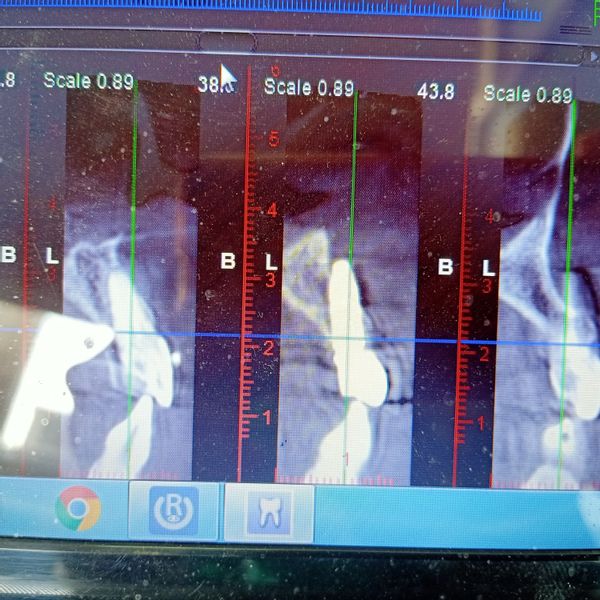
This is an immediate implant was placed seven days ago. The panorama represented good positioning for the implant but come beam was showing major defect in the implant placement in a more buccal direction causing a fenestration apically and a little labial bone present. How would you manage this?
DrV comments:
Well, Remove - Graft - Put a new one.yasmin comments:
What if primary stability was 40 Can I do GBR only on the labial bone?Jim comments:
It's too far to the Buccal. Take it out, maybe use a slightly smaller diameter, and follow the Palatal wall, as Tim said, and do GBR over the opening. Prosthetic restoration will go a lot easier for you, as well.Tim comments:
Looks like you followed the root of the existing tooth instead of following the palatal wall which is a common mistake when placing anterior immediate. Not really sure why it would be recommended to remove and graft because there is plenty of bone you just missed it. Doing GBR on an avascular surface is questionable. I would leave it alone and if there is adequate thickness of connective tissue this may not present a problem. By no means should you remove it just because a radiograph suggestsTim comments:
In all honesty the fixture is probably 2-3mm longer than necessary and all you have is an ugly image while the implant should be fine. Leave it alone and chalk it up as a learning experience!!!Rand Ollerton comments:
Dr. Ernest Lee has a technique that may be helpful, the "S.M.A.R.T." graft. I have not taken his course, but he has had results.Google: PREDICTABLE COMPROMISED IMPLANT RESCUE TECHNIQUES
Dr. Ernesto Lee’s S.M.A.R.T. method provides an alternative for the treatment of complex scenarios including the management of compromised implants.
mbarr comments:
Remove the implant now and than rethink how you are going to graft this problem; just filling the “socket” with allograft will probably not work. Than consider taking two steps back and self-asses how you ended up with this situation. Several other observations- the temporary is in function, the implant is too wide for this location and what about all those rotten molars in the mandibular posterior?Dennis Flanagan DDS MSc comments:
Lift a full thickness flap debride the area. The adjacent tooth looks like it may need an apicoectomy/retrograde filling, if so do that then. Place a particulate osseous graft material 4mm thick, cover with two layers of a collagen barrier so no need for retaining screws. Rx antibiotics. Primary closure with non-resorbing suture.Scott F Bobbitt DMD MAGD comments:
Hey Dennis! I know you've done way more of these than I, but isn't the apex too far out of the natural alveolar housing for a successful veneer graft? I would think that the volume of extraosseous exposure would be the limiting factor for success, vs removal and replacement with shorter, smaller diameter implant after GBR.Raul Mena comments:
This is a no brainer, Remove the implant, Graft and then after bone remodeling place the proper implant in the right position. It happens, don't get discourage.