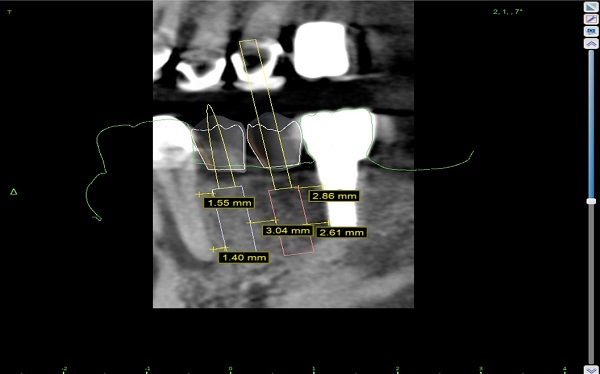
I would like some help with this case. Astra EV implants planned for lower left. I'm using 3.6mm x 11mm implants due to the space available. Even so, I cannot achieve ideal spacing between implants, but it's close. Can I proceed with the placement since it's pretty close or should I replace the forward implant, or both, with the next size smaller implant which would be a 3.0mm? I am also concerned about the apical positioning of the implant in the 2nd premolar position(to achieve proper emergence profile of the restoration)-will crestal bone be lost around the existing implant distal to it?
Another possible option would be to lose #22 since it has an abscess and then place 2 larger diameter implants and do a bridge. Patient would rather not lose #22(it's planned for endo tx with specialist) and I tend to agree with this.
Any feedback would be much appreciated.
mark comments:
can't tell much about 22 is that a large lucency? I would take care of 22 before i did any implants remember phase 1 treatment of disease before phase 2 replacement of teeth
Paul R comments:
I agree about being sure tooth #22 is healthy BEFORE doing any implants. From your CBCT it appears that you have adequate inter implant space of 3 mm and adequate distance, 1.5mm between implants and natural teeth so I would proceed with this treatment, once tooth #22 is healthy
Junaid comments:
After hopeful successful endodontic treatment of LL3; may be just place one implant to replace LL4 and construct a 3 unit implant retained bridge using the existing implant on LL6?
Could save major palpitations for you at the surgical phase!
Benkless comments:
Wow, I have to admit I never even thought of that. I think that is a very sound option. This is why I like this forum, thank you.
Matt Helm D.D.S. comments:
Considering the excessively large radiolucency mesial to #22 you must adress that first AND be sure it's resolved completely and that the tooth is asymptomatic before you proceed with any implants, because the loss of 22 will drastically alter your implant tx plan. IMHO I tend to doubt that after treatment the #22 will remain viable and asymptomatic for too long, but we've seen worse and, one never really knows in this profession with these things. Also, I concur with Junaid that one wider and more stable implant with a bridge to #19 would be a better, more conservative solution, which can also be adopted if the #22 is lost. In any case, this mandible certainly has sufficient bone width for wider implants than the 3.6 mm you're planning, and it would be beneficial for long term implant stability. Some would opt for immediate extraction of the #22 and replacing it with an implant, with a second implant in the #21 position and a bridge to #19, without even worring about trying to save a #22 that has only a 50% chance of succeeding. In fact, that may be the most eficient, expedient and longest lasting solution of all, as well as the most cost-efficient to the patient. Let's not forget that even if the #22 is saved for now, this will require an aditional investment from the patient (for the #22) and there will come a time when it will be lost, and that will mean another implant anyway. This way, the patient saves not throwing good money into a bad #22. Something to think about and to also present to the patient. Good luck.
Matt Helm D.D.S. comments:
Nice case presentation, with all the pertinent details. Congrats!
Benkless comments:
Very well thought out advice, I appreciate it. Endo tx is scheduled and the implant is on hold. Pt. Understands all risks and is ok with possible future implant to replace 22 if it fails, but if it makes it will be a good situation for pt. Implant bridge from 19 to eventual implant 21 is planned.
So how long after endo tx is it safe to place the implant? Obviously needs to be sx free, but what about the lesion- should wait to see radiographic decrease in size? How long could that take?
Hosseini comments:
After Endo, I would place an implant in the area of 20 (4.2 or 4.8 mm diameter) and after 3 months fabricate a cantilever bridge for 20, 21. Leave 19 alone. Placing 3.6mm implants for 20 and 21 would work as well. I wouldn’t cantilever off of a 3.6 on the posterior.
molarfix@cs.com comments:
Extract 22, bone graft, place 3 implants sites 22 21 20. If using narrow implant, splint them all.
Janci comments:
Primary RCT has only a 50% success?? Oh I see, its an implant forum.