I placed an Osstem Ts3 4x10mm implant in 45 area 4 months back. During 2nd stage, after placing a wide healing cap for 7 days, I took open tray impression with a special tray fabricated by the lab. Once the crown came, it just wouldn't fit. I initially thought maybe the crown is tight mesiodistally and reduced the crown mesiodistally but still the crown wasn't even close to snap fitting. So I took a closed tray impression the 2nd time ,took an xray to check fit and asked the lab to pour it. After pouring the lab said that the 2nd model is exactly same as the 1st one. So this time I planned to remove the crown from the abutment and try to place the abutment with a transfer key. The abutment didn't seat correctly.So I removed the key and placed the abutment correctly.After placing it, I have taken an impression of this abutment. The abutment used is hex tibase abutment for screw retained crowns.What confuses me in this case is a few things- 1)If the impression is wrong,how is it possible that the xray shows the coping fully seated and if while picking up the coping the movement happened,how is it possible that both the open and closed tray impressions have exactly the same mistake as both the casts are the same? 2)What do you think is the reason that the crown is not seating on this implant?I have changed the abutment 2 times already .Please check xrays. Impression was taken with putty and light body both times.

rogr2000 comments:
I don’t see any locking mechanism on the titanium base. For sure movement occurs. It looks like Sirona Ti Base. I believe the Ti Base was not placed in the correct placement in the impression. Thus your hex is rotated hence your predicament.XYZ comments:
The 1st impression was an open tray so the coping was picked up in the impression.I screwed the analogue to it.When I do that I hold the analogue with my left hand to prevent rotation while I tighten the screw on the coping.The patient cane 7 days later for me to screw the crown however the crown didn't fit.So this time I took a closed tray. I placed the coping into the impression.7 days after this the crown again didn't fit.I asked the lab to decement the crown from abutment and give me a key for it.When I tried to place the abutment with key it didn't sit(the 1st xray).I removed the key and tried to slightly rotate it.Thats when it sat(2nd xray).How is it that both the impressions were wrong in exactly the same amount to make the casts exactly same(confirmed by the lab that both casts are same).Could there be an issue in the milling machine with an error?But then the crown shouldn't seat in the cast which it doesIan comments:
You should have a custom abutment made or the bone likely needs to be profiled.XYZ comments:
This maybe a reason however 1 question still intrigues me.If the bone needs to be profiled or the custom abutment needs to be made,how did the abutment fit on the implant after removing the key which the lab had given me(evident in the 2nd xray).fordent04 comments:
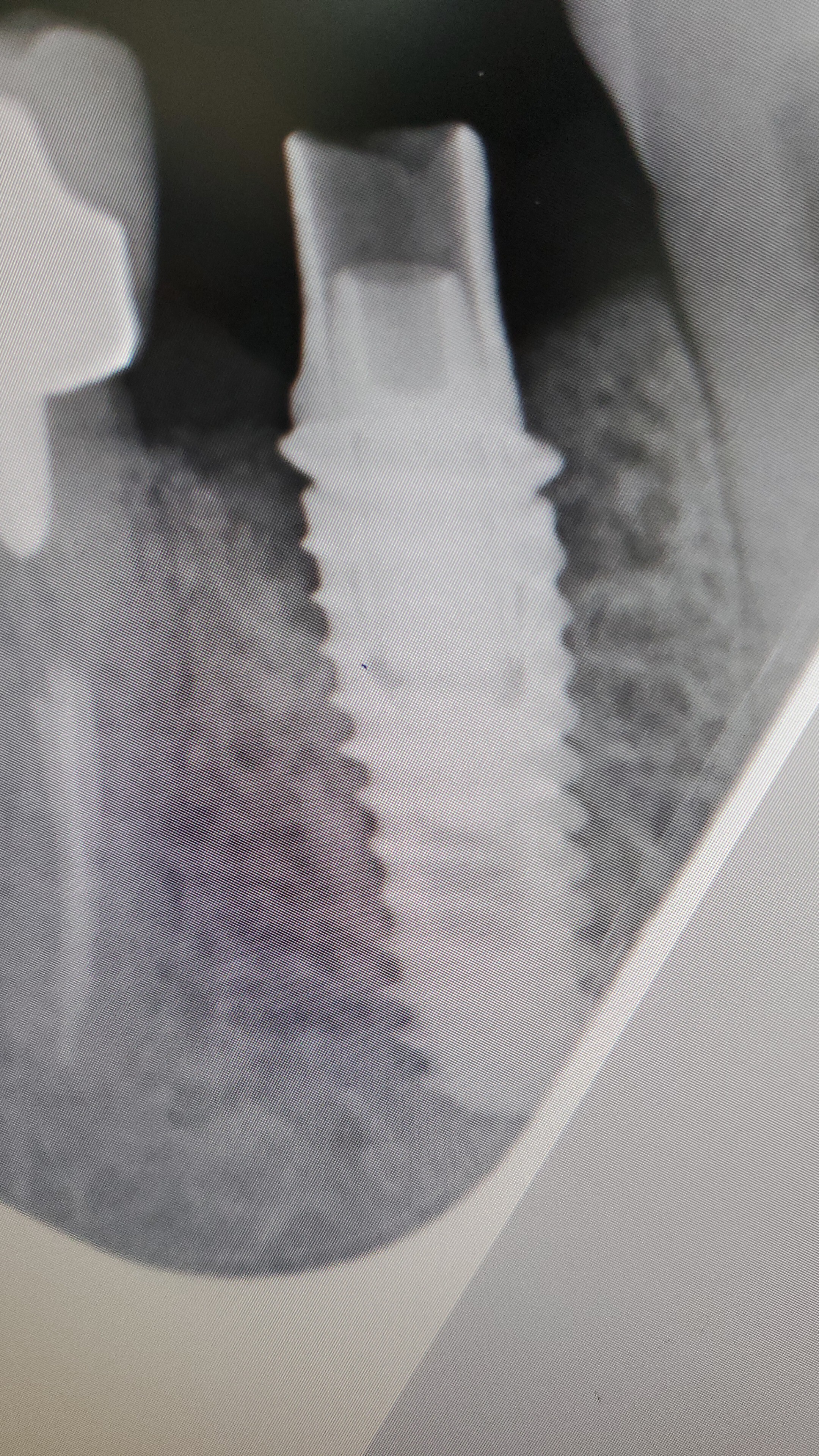
The first x-ray clearly shows the abutment hex does not fit correctly. This means your first impression was distorted if your impression coping was placed correctly. This was the reason of your second impression and transfer key were not fit correctly. This type of distortion is rare but happens. I suspect this happens when we connect an analog to an impression coping. If you could provide any x-ray image taken with an impression coping of your first impression then we could tell whether the impression coping was properly connected.XYZ comments:
The 1st xray is of the abutment when placed with a transfer key(its unseated).The 2nd is after I removed the key and rotated the abutment to fit it.The funny bit is that this was made on the 2nd impression(both impressions being exactly same)dale@drdalegerke.com comments:
does the abutment and crown fit on the lab model WITH the silicone ging replica in place? if not then that is your likely problem. what often happens is that you can take an impression accurately using a coping because it is usually a narrower diameter than the ging access hole created by the healing abutment. but then the lab uses a wider abutment and adds more volume/diameter when they make the crown - so the emergence profile is ideal in their mind (they usually remove the silicone - so now i insist they always make sure the crown fits before they remove the silicone) unfortunately the soft tissue "push back" can be much more than expected (you would think you could push the ging out of the way). thus you need to either reduce the emergence profile width on the crown or alternatively make a "slice" cut (mesial-distal) then insert the crown. the ging will open and allow the crown to click in. the ging will quickly heal after a few days.ajv68ss350 comments:
I have had a similar situation. The final result was the implant lost stability and was failing , but did not show on any X-rays. I went thru all the comments that were made with no success. After using a laser to fully expose the complete platform of the implant and placing an impression transfer , then using finger pressure to move the impression transfer slight movement of the implant could be visualized. The patient had no symptoms .40yrvet comments:
Seems like bone growth on the mesial with accompanying additional gingival height is preventing crown seating. You can try to use a bone mill, or flap and use a surgical bur to obtain a reduced tissue profile. Try the crown in during the surgery to obtain a clearer view and test out the reduction. A better approach is a custom abutment with more distance between implant platform and crown margin for proper crown seating and future hygiene. This will develop periimplantitis if there is not enough physiological space between crown and implant.XYZ comments:
Thank you for the reply.I think this is the issue