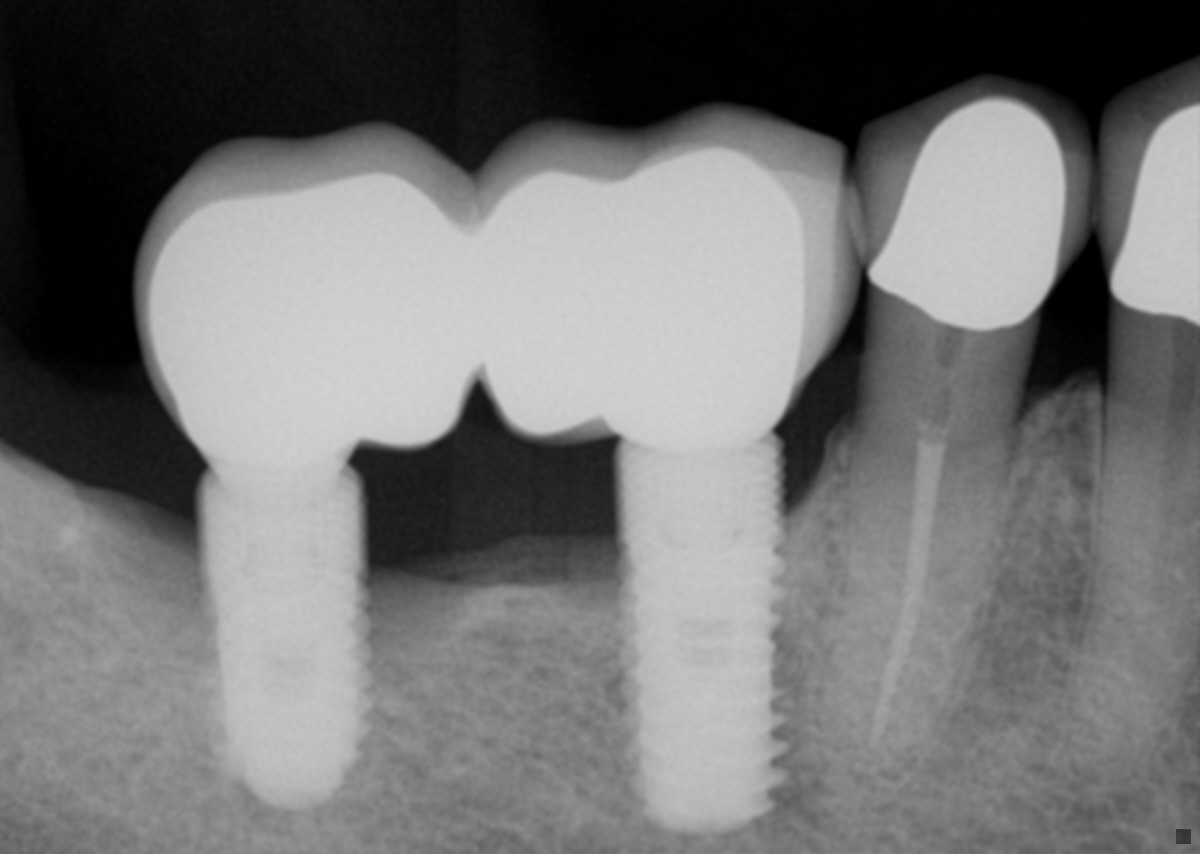
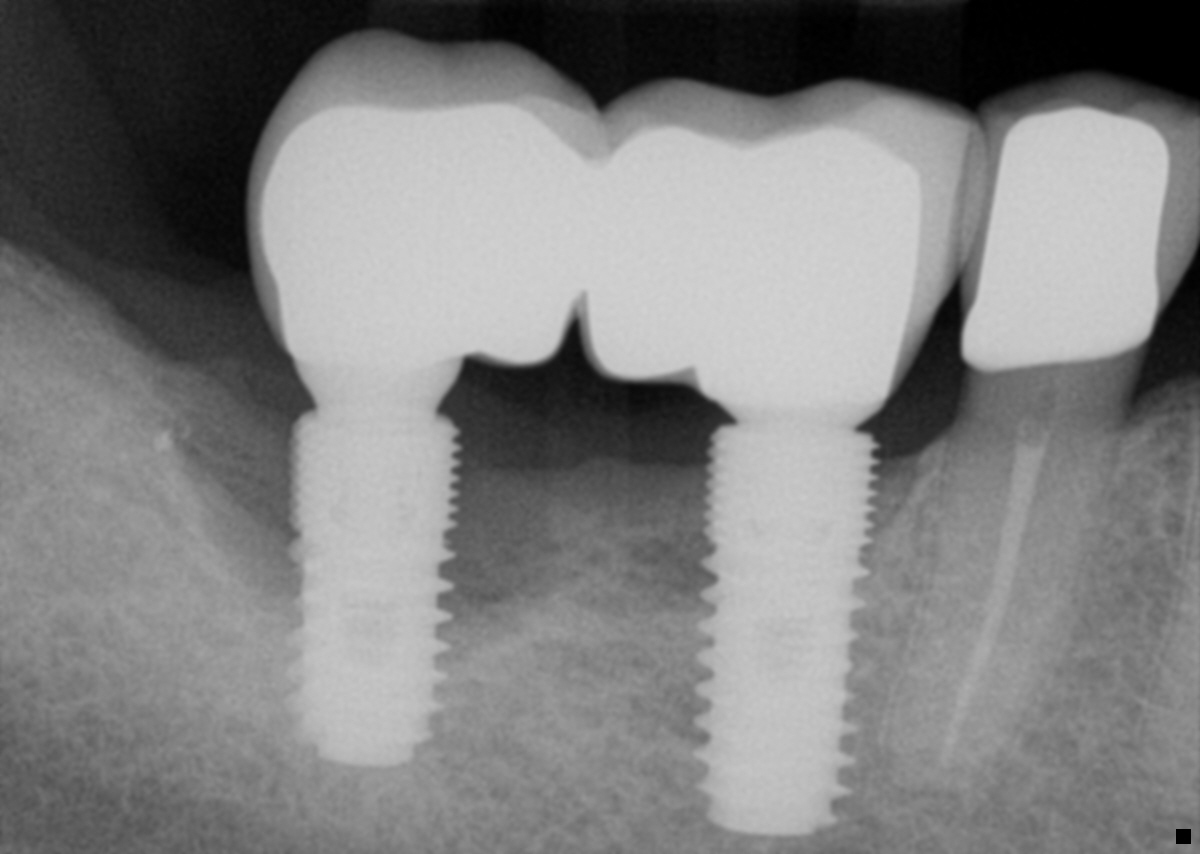
71 y/o male with failing implants in the lower right (#30 and #31). Most distal implant(#31) has suppuration. Would like to know if you would remove both implants and rebuild the area with GBR(allograft/titanium reinforced PTFE membrane/tacks), or try to keep the mesial most implant(#30) and still do GBR with burying the implant?
John T comments:
Difficult to comment without knowing your patient's occlusion. I assume only the distal implant is infected. If so, I would be inclined to keep it simple: (a) Section the bridge between LR7 and LR6 and remove the LR7 fixture and distal half of the bridge. (b) Leave the LR6 implant and crown in situ. The prognosis for the LR6 implant is not brilliant but it may function for several more years. Trying to turn the clock back on the LR6 implant by conjuring up alveolar bone with allograft/ titanium reinforced PTFE membrane/ tacks, etc (aka "fairy dust!"), would carry an unacceptably high failure rate.Adrian comments:
Thank you for your opinion. Both implants are in full occlusion opposing upper 2nd and 1st molars. So pt. desires to restore this function eventually. Does this change your opinion at all? Would you still just explant distal implant and leave that site alone or try to graft that area?Chris comments:
Both explanted. Rebuild ridge. Go again , if patient wishes....Adrian comments:
Thank you. My first inclination is to rebuild entire site also. Pt. currently functions on the entire implant bridge and his desire is to restore that function if possible with a fixed solution.robertsalisbury comments:
The issue that start a lot of these problems is that conical connections that are bridged and direct to the implants have leaking seals. Individually the seal is fine but splinted will ensure that they will not connect and seal properly. Consider flat top implants in posterior or increase your cost and put on costly multi units to seal independently first and then a bridge to the flat top. This now becomes a possible aesthetic issue as it raises the metal upwards. Its an engineering misfortune on conical implants that have "slippage vertically upon torqueing" that steep conicals have. Astra, Conelog, are demons in this category with long conicals. Perhaps unload, seperate, and put the Mesial one back on and try to clean up and regenerate. Cheers and good luckDr.Mahijeet Singh Puri comments:
If the implants have xero mobility , this is a classical case of peri implantitis. Remove both the crowns. Place cover screws on both. Do GBR with good quality bone graft and resorbable membrane. Stick to the principles of bone regeneration. Use PRF if possible. Suture with resorbable sutures tension free. wait for atleast 4 months. Very important, do not probe the grafted area through the mucosa. Let it heal, let the attached gingiva form. See the result. Put the patients on tetracycline 500 twice daily for 21 days along with pain killers for 5 to 7 days.Adrian comments:
Good advice, thank you. What, if anything, would you do to the exposed implant surfaces before placing the graft?Tim comments:
IMO removing both implants would be like killing a fly with a hammer. I would start by accessing the abutment screw on #31 to remove the crown and place a cover screw/healing abutment. After some time it may still require explanting but I seriously doubt that any complex GBR/Titanium Mesh/Muscle flexing regenerative procedure will be required as the human body, even in a 71 y/o, has an amazing ability to heal without unnecessary manipulation. The other fixture #30 looks fine and I would leave it alone though you might consider redesigning new restorations to correct what appears with this image to be a food trapping pseudo pontic. If you must remove #31 I would consider replacing it in a more mesial position to correct that IP area.guest comments:
Good LAPIP case.