59 year old female. About a year ago I extracted #3 and placed a socket preservation bone graft upon referral by general dentist. The dentist then placed the implant (see images). The new dentist who took over the general dentist practice told patient that the implant is malpositioned and needs the implant removed, re-grafted, and subsequently a new implant placed. I am planning to raise a flap, remove the implant, and graft. I think a titanium mesh would be the best approach in this case. Any recommendations? Thanks.

CARLOS BOUDET DDS comments:
It is true that the implant is not positioned correctly, however, the implant is in the posterior region of the mouth and it can be restored by compensating for the malpositioning with the design of the restoration. Also if you consider the damage to the area including the possibility of complications from the sinus and explain this to the patient, I think the benefits of restoring the implant as is outweigh the new revision surgery.
Good luck
Dr matt comments:
Slight angulation/position issue. Not sure I’d consider removing and redoing. Patient is not mine so I am not seeing clinical issues, but without any other problems leave it alone. May be getting a little picky.
Zachary comments:
So we reach a part of implant dentistry that is difficult. When to removed a integrated implant due to poor positioning.
This case appears to be close to unrestorable. But before putting your patient through additional surgeries and in this case a proposed titanium mesh you better be sure.
It’s tough to judge with only radiographs and no clinical information, but I would try to restore first if reasonably possible.
Reasonable: contours, shape, size, emergence profile, occlusion, etc.
If I thought any long term issue would arise from restoration being less than ideal, or patient would be unhappy and in my office every week, then I would take out the implant using a removal kit from one of the major manufacturers to reduce amount of bony destruction and get new implant into an ideal position.
Implant dentistry....... It’s easy until it ain’t!!!!!
John T comments:
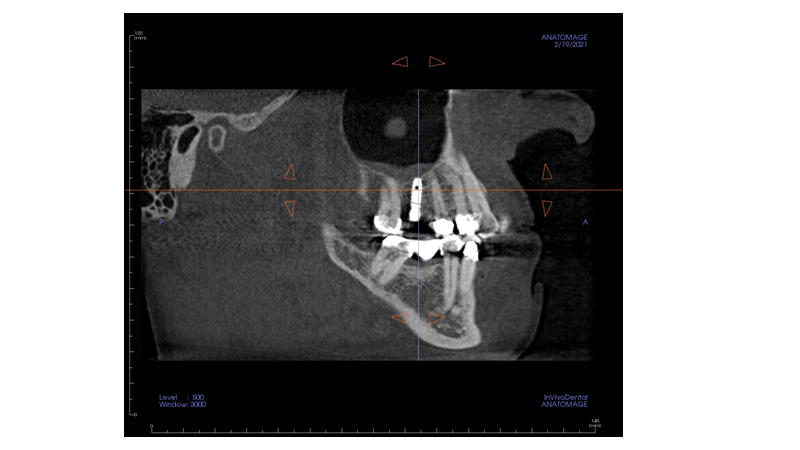
Sorry, I can't see the problem. We only have x-rays to judge from, but the implant fixture is the correct length, appears to be reasonably aligned bucco palatally and has good bone coverage buccally and palatally. It is not exactly equidistant between the adjacent teeth mesio-distally and is angled slightly distally but there's nothing here which can't be overcome with a custom-made abutment - of which there are a number of systems now available. Don't be tempted to interfere with it in any way.
I’m more concerned by the crown on the lower right second premolar. The sagittal CT appears to show it hovering in space.
Drwhytfang comments:
I agree I’ve seen a lot worse While not perfect can be easily restored I thought this post was like Ann April fool prank at first
mmvalenzano comments:
Before CBCT would you remove this implant, NO, the risk of further surgery, and complications. It would be prudent to restore as is with angled attachment, if and when it fails then redo, but not now for a little less than ideal position, I have had this type of implant survive over 35 years,what else do you want?
rpfitton comments:
While not ideal,the implant can be restored given the information presented here. My guess is the second dentist does not have much experience with implants otherwise he would know trying to remove that can cause more damage. The cure being worse than the disease.
mahijeetsinghpuri comments:
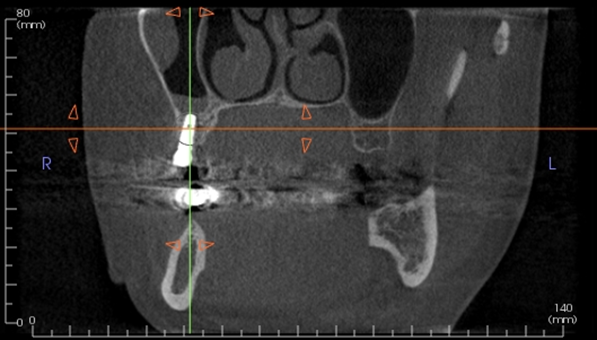
I don't think the angulation is the big issue here. There seems to me at least 3--4 mm of crestal bone loss on the mesial side which is developing into bone loss going onto the distal side ,developing into a perimplantitis.
Is there any mobility
What is the ISQ VALUE
IS THERE ANY BOP the pockets
If all the factors remain favorable
then angulation is not the issue
Go ahead and place the crown.
Tim comments:
Could someone please advise me as to why this implant is even considered non-restorable. Unless there is something more which is not presented here than I believe removing this constitutes malpractice.
Dr. Nondas comments:
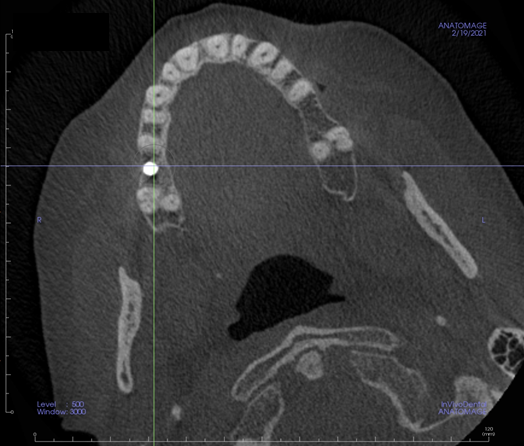
The cbct shows that the implant is positioned more distally and more bucally than the ideal position. However, it is placed deep enough to create a good emergence profile and avoid food trapping. Trying to remove it with trephine drills will damage the buccal plate. A CTG buccally would help the thin buccal plate to be preserved. So I vote to keep the implant, place the CTG, let it heal and restore.
Dr Zoobi comments:
Looks very restorable to me. What’s wrong with restoring and monitoring? I don’t see the logic behind replacing.
mbarr comments:
insufficient clinical information - just a little more detail needed to answer this important question
vertical bite wing, intraoral pax, perio info and why the fluid level in the sinus in this quadrant. Nice cbct and pano though . Thank you
Dr JohnW comments:
Just a general observation. Why is an implant that is off plumb by about 10°, “malpositioned” when All-on-Four implants are intentionally placed 30° off plumb and called “normal”?
The potential peri-implantitis is much more concern that the “misalignment”
A good lab can correct this problem, and provide a great result.
Aquiles comments:
I agree with some of the other blokes on this one. Yes. The implant is not perfectly placed. But the complications of removing, can far more complicate your life more than restoring the thing at this point. I’d restore and get what you can out of it.
B W comments:
Just going off the radiographs is tricky, Malposition and angulation can be over come with correctly selected custom abutments and angled screw with a good contour crown. Need to weight up risk and benefits and justify why you should put the patient through such a major intervention. All in the patients best interest and if clinically it shows it should be removed then so be it. My concern is the thickening of the mucosa in the RHS antrum which could be due the implant. How do you plan on removing the implant will define how plan on grafting afterwards as a simple reverse torque may just need some CS and closure.
DrV comments:
Nice to see the pre-op Xray from before you removed #3 and graft it. Apparently has sinus pathology.