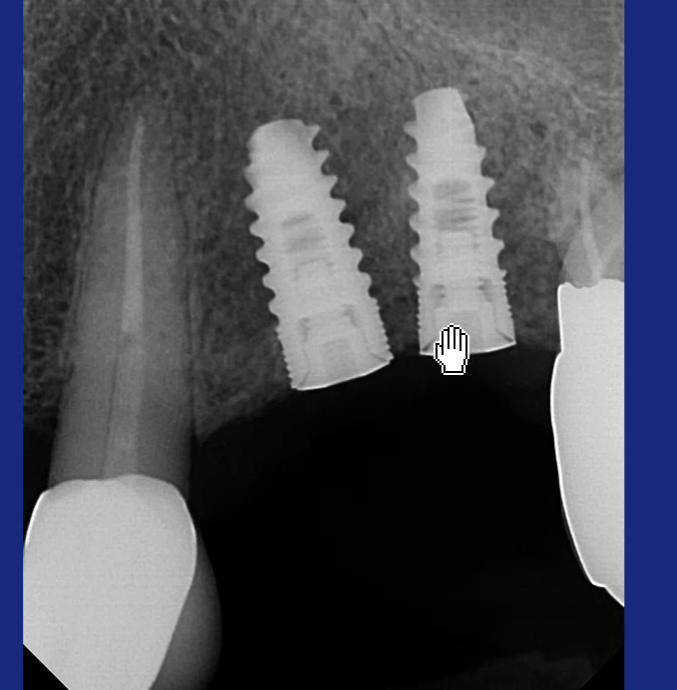
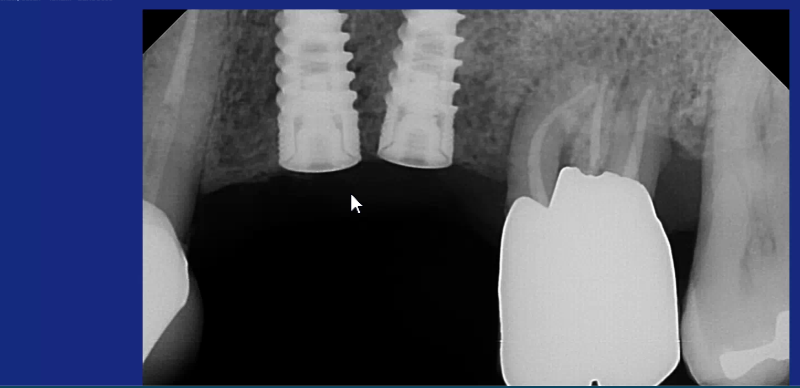
These 2 implants were placed 2 years ago and are fully integrated. There angulation and proximity are very close. I am planning the secondary surgery but anticipating difficulty. Please comment on how you would approach this restorative process.
Andrew UK comments:
Restoring them is easy enough for your technician using angled abutments. The difficult bit is taking an impression. I would try in your open tray impression copings and use a dental bur to shave off the distal of the anterior coping and mesial of the distal coping until you can see clear space between them when they are fully seated. You'll probably have most of the retentive parts of the copings still intact. If you haven't, you can use pattern resin to splint them together using a bead on technique. Then just take your impression in an elastomer like polyether and you're done. Your techie will sort out the rest.dale gerke-prosthodontist comments:
in general these comments are correct. however the previous comments have relevance. the positioning is not idea and exemplifies the desirability of using a surgical guide. nevertheless this situation can be restored albeit not ideally. however my tip (from bitter experience) is not to splint copings because either it will make it very hard to withdraw the copings, or considerable trauma will be caused to the patient's soft tissue, or the splinting resin will crack (by necessity to remove the copings) and the position of the copings may therefore be distorted. i have found using the correct polyether will be satisfactory to retain the copings accurately. by using just the rubber impression allows enough flexibility to remove the copings without too much trouble. however there are a few tricks you might need for restoration. use a standard abutment for the distal implant and a redirectional for the mesial. obviously the lack of interproximal space will require "straight" sides and so probably it will be best to design the crowns so the mesial crown is inserted first then the distal. this is because the path of insertion will probably be easier this way. the problem with this type of situation is getting a tight contact interproximally which is why i suggest you ask the lab to construct the crowns as suggested above.Andrew UK comments:
Yes I’m sure that’s right. Only splint if you’ve had to remove all the retentive features from one of both of the impression copings in order to get them to seat passively. It will indeed make them more difficult to remove and you’ll just have to hope for the best. I suppose you could try to use pattern resin to increase the retentive features whilst keeping them separate. Good luck anyway 👍Guy Nash comments:
Just make sure your closed tray impression copings are seated completely. Verify with xray. Take impression and place implant analogs onto copings and make sure they go into the impression accurately. Lab should now be able to make angled abutments to help with seating. You can splint them together but I would ensure that the lab gives the patient room to get between the crowns for hygiene.BroMike BroMike comments:
Did you mean you don't splint the impressions copings in general or just don't splint if the implants are off angle too much?Dr. Michael T. comments:
It’s not only restoration problem, since you will get no papilla between your implants. Still, although not perfect, I would place two MUA, change angulation and convert to tissue level, then take impression. Finally splint the two crowns.BroMike BroMike comments:
why don't you use custom or angled abutments?VP comments:
remove mesial implant :wink:Rob Tilon comments:
I would be honest with the patient: propose a better plan. Take out the molar, place an implant in that site, remove at the same time the implant at position #5, and make subsequently an implant bridge. I would not charge for the new implant……Barrow Marks comments:
I thank all my colleagues for your suggestions. This comment is for Andrew. I like your solution however I feel that the length of the open tray impression coping‘s will not allow me to seat two at the same time. I fear That the trimming of these coping will ruin them. Would you consider two straight stock abutments that are trimmed to make room between them and then take a conventional elastomeric impression?Andrew UK comments:
Yes, you’re right, that might be a problem which is why I said that you might lose your retentive features of your impression copings. I would try it and see though. I don’t think that they look too bad from your radiographs and the chances are that they might diverge bucco lingually too. That will help you to get them both in place whilst maintaining as much retention as you can on the copings. Yes, you could use stock abutments but they may not be retentive enough and strip out of the impression as you remove it. Also, in most systems, there is a choice of impression coping lengths which might help. Anyway, I would give it a go and see how you get on.Barrow Marks comments:
Would you also consider one custom abutment and one PEEK abutment considering that the PEEK abutment will be very easy to trim. Or possibly two PEEK abutments and an elastomeric impression?Indraniil comments:
1ST YOU WILL.NEED TO DO A 2ND STAGE SURGERY AND PLACING HEALING ABUTMENTS.THAT SHOULDNT BE AN ISSUE. AFTER THIS YOU NEED TO TAKE AN IMPRESSION.YOU HAVE 2 OPTIONS,EITHER USE OPEN TRAY IMPRESSIONS AND SHAVE OUT THE PART OF THE IMPRESSION COPING WHICH IS TOUCHING (TO MAKE SURE COMPLETE SEATING OF THE COPINGS).THE OTHER OPTION IS USING TEMPORARY COPINGS AND USING THEM FOR AN IMPRESSION.FOR THE ABUTMENT OPTIONS ASK THE LAB TO USE A DYNAMIC ABUTMENT TO CORRECT THE ANGULATION.GOOD LUCKRand Ollerton comments:
Use two stock abutments, one straight, one angled and place on the implants. Take a closed impression. Use the stock abutments as Impression abutments and attach analogs and pour a model. Restore with modified custom abutment or custom abutments for cemented restorations or UMA for Screw retained.J L Watters comments:
The molar has a poor prognosis, in my opinion, with advanced furcation and osseous defect on the distal buccal and widened PDL on the mesiobuccal; you could remove it, place a wide implant and then bypass your center implant and make a fixed implant bridge. Just putting that out there.