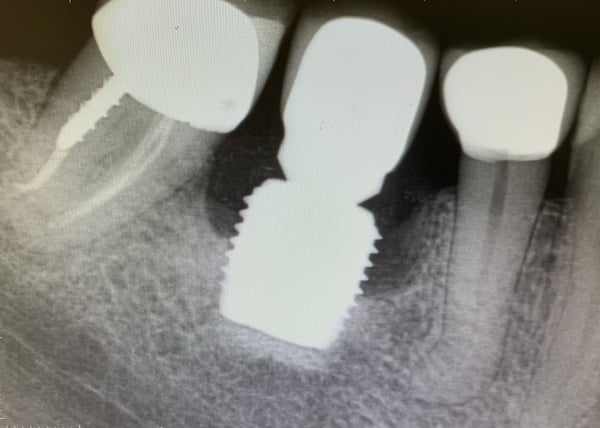
A colleague of mine sent this radiograph inquiring as to what can possibly be done to address the bone loss around this implant. What would you propose in this situation? Do you think this could have been avoided for this particular implant or was this inevitable?
timcarter comments:
Who knows but I would suggest diving into the literature on the complications associated with wide implants. I believe that these wide fixtures remove too much vascular bone during the osteotomy and thus rely on avascular cortical bone for stability. The lack of vascularity makes them vulnerable to such conditions.
drdangober comments:
I agree. An implant as wide as this should not be placed in a premolar site. There just isnt enough bone width to support it so I think an outcome like this or similar to this was inevitable. And to add insult to injury, what will need to be done to get this out is going to be very traumatic!
gregkammeyer comments:
I agree also. I use 6mm implants routinely for molars and seldom use a larger diameter.
drag comments:
Many wrong things with this implant. As stated, the wide diameter created bone lost. How is the soft tissue? Probably deficient also. Best option, remove it, vertical graft to the bone peak of adjacent teeth, enhance soft tissue and place smaller implant. If you do titanium plasti on the implant, you may save it for a little while but will be even harder later to gain bone.
Impossible to graft around this expose titanium
admiral518 comments:
Hi. From the xray I assumed it was a molar. Having at least a panoramic could provide other clues.This question requires further info. For instance.1-How long ago was implant placed. ie 2mo. ago vs 20 yrs ago would lead to different recommendations.2- is it symptomatic? Pus on palpation? Mobility? Pocketing? Pain? Smoker?
If placed years ago and no suppuration dont touch it.
How old is pt? If he's 70+ vs if he's 30 and just had it placed 2 yrs earlier, It would be handled differently.
Getting back to the lack of a panoramic. Its difficult to advise without seeing the overall occlusion. What if the pt is missing occlusion on the left side? Even if you replace this implant with a smaller diameter one it will still get beat up. No tth is an island. Its group function. Spread the force of mastication over as many tth as possible. Again need a pan. and more info.
ttmillarr comments:
Yeah, probably take it out and graft while you still have some interproximal bone, maybe use a tent screw. Looks like you have some vertical bone below the existing implant to use too.