Early peri-implant bone loss: normal response?
Last Updated: Apr 09, 2014
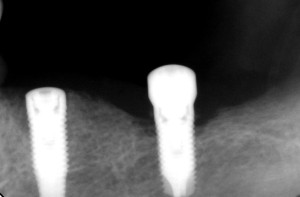
I have a 67 year old female patient who smokes 10-15 cigarettes a day. She has excellent periodontal health. I installed implants in an edentulous area in #19, 18 areas [mandibular left first and second molars; 36, 37]. On the 1 month recall the healing abutments were exposed. I changed the healing abutments. The radiograph showed rapid bone loss around #18. Is this a normal response of the bone? Could this bone loss be due to cigarette smoking or overheating the bone when I drilled the osteotomy site?
![]peri](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2014/04/peri-e1397071061154.jpg)
{kind=link}
{kind=link}
![]pano](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2014/04/pano-e1397071083729.jpg)
{kind=link}
{kind=link}
13 Comments on Early peri-implant bone loss: normal response?
Anton Andrews
04/11/2014
CRS
04/12/2014
Ed
04/12/2014
CRS
04/12/2014
Ed
04/13/2014
CRS
04/13/2014
DrT
04/15/2014
David Vaysleyb
04/17/2014
David Vaysleyb
04/17/2014
CRS
04/17/2014
Gregori Kurtzman, DDS, MA
04/22/2014
DrD
04/22/2014
Featured Products
Classic 50/50 Mix
Promotes osteoconduction
Provides structural integrity
Convenient Syringe!
50/50 Cortical/Cancellous
Available in 3 sizes.
Eliminate hassle of mixing particulate grafts
Sold in packs of 5 or packs of 10.
Proven safe, and clinically effective
Resorbable collagen membrane derived from purified porcine pericardium
Fast hydration and excellent tensile strength
Good adaptation to various defects
Excellent tear function and duration
100% allograft
Eliminates mixing hassle
Moldable after hydration
CRS
04/09/2014