Failed Immediate Implant: Feedback on this case?
Last Updated: Jun 28, 2012
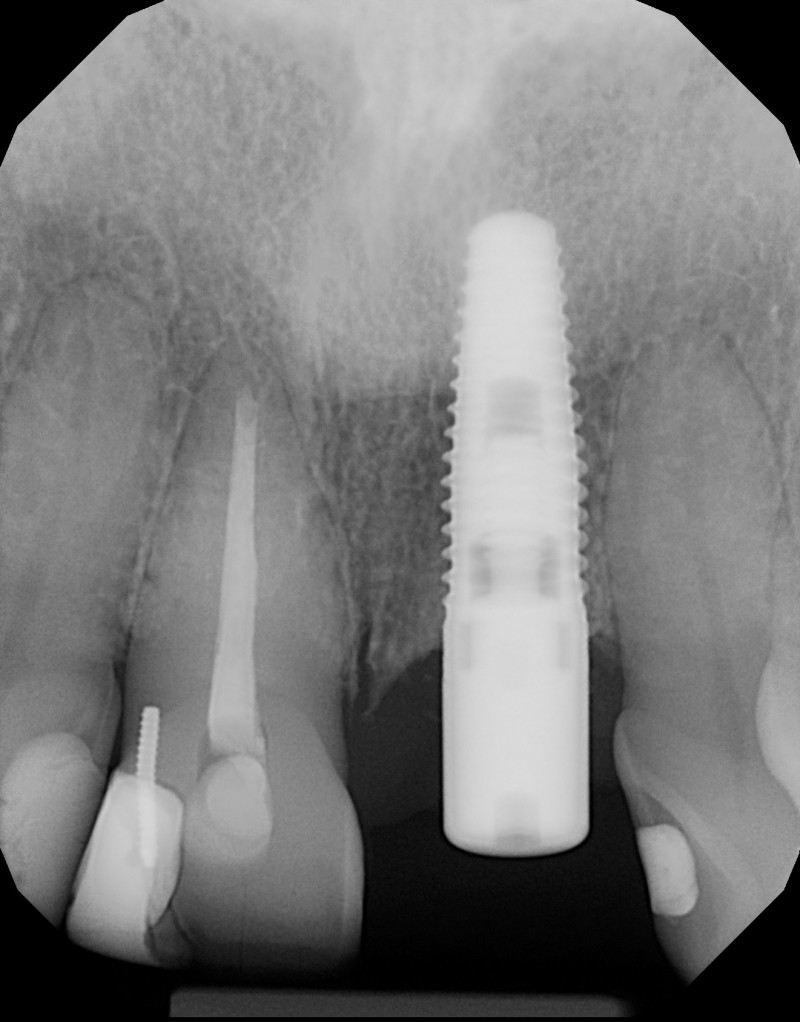
The case you see below is a failed immediate implant tooth # 21. I placed the implant after atraumatic extraction in the palatal wall and left sufficient space between the implant and the labial wall and there was no pre-existing infection, rather a split tooth situation.
Everything looked radiographically and clinically fine until the patient returned after having the screw retained temporary in place for 6 weeks (9 months of osseointegration). At this point the lesion you see on the labial appeared. I then had another CT scan done and it appears as though there is little to no labial plate. My plan is to flap and graft the labial area. I think retrieval of the implant would be difficult as it is well integrated elsewhere.
I am not sure with such a graft if I can leave the temporary in place or if I should place a cover screw and let the site close over for optimal graft results? Any feedback on this case would be greatly appreciated.
(click images below for enlarged photos)
Healing Collar 7 Months
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2012/06/7-months-healing-e1340888337914.jpg)
{kind=link}
{kind=link}
Temporary crown 9 month’s
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2012/06/temporary-ay-6-weeks-e1340888368410.jpg)
{kind=link}
{kind=link}
Healing Collar 7 months
![]healing-collar-7-months](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2012/07/healing-collar-7-months-e1341352405557.jpg)
{kind=link}
{kind=link}
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2012/07/healing-collar-7-months1-e1341352433774.jpg)
{kind=link}
{kind=link}
15 Comments on Failed Immediate Implant: Feedback on this case?
Brent MacDonald
06/29/2012
Greg Steiner
07/01/2012
Sam Jain DMD
06/29/2012
Brent MacDonald
06/30/2012
Dr. Omar Olalde
06/30/2012
David Chan
07/01/2012
Sam Jain
07/01/2012
Brent
07/01/2012
OsseoNews
07/02/2012
DrT
07/03/2012
Brent
07/03/2012
osseonews
07/03/2012
Gregori M. Kurtzman, DDS,
07/03/2012
Dr. Alex Zavyalov
07/04/2012
Featured Products
Classic 50/50 Mix
Promotes osteoconduction
Provides structural integrity
Convenient Syringe!
50/50 Cortical/Cancellous
Available in 3 sizes.
Eliminate hassle of mixing particulate grafts
Sold in packs of 5 or packs of 10.
Proven safe, and clinically effective
Resorbable collagen membrane derived from purified porcine pericardium
Fast hydration and excellent tensile strength
Good adaptation to various defects
Excellent tear function and duration
100% allograft
Eliminates mixing hassle
Moldable after hydration
Greg Steiner
06/28/2012