Unscrewing Dental Implants
Sam, a dentist, asks:
I have placed 4 dental implants in the 28 ,29, 30 and 31 areas. The patient
called me the day after surgery to complain that his lip and chin are
still numb.
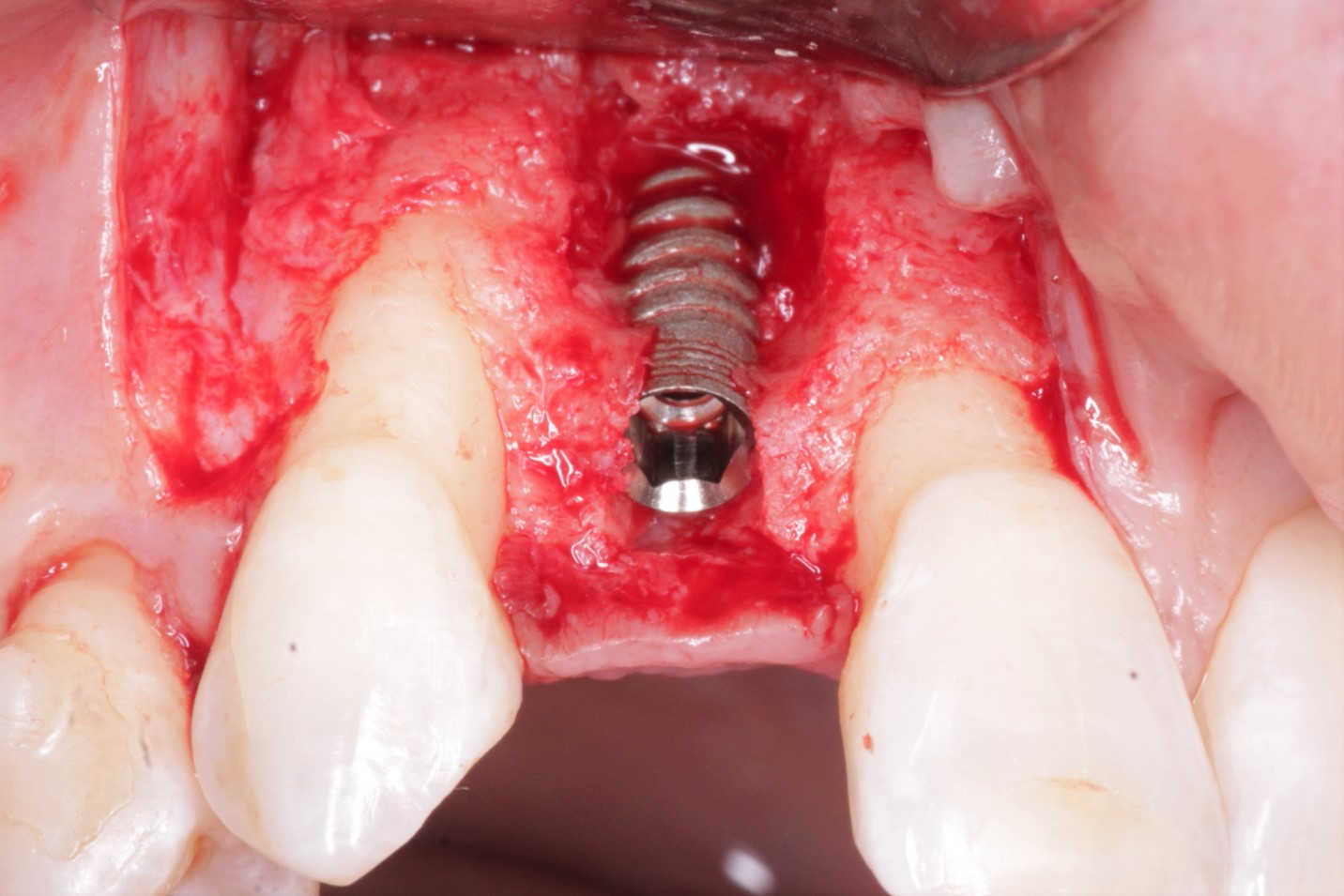
I had the patient come in and I unscrewed the dental implants in
31 and 30 areas by a thread or two. The patient immediately started
having more sensation in his lip and chin. The sutures opened shortly
after and the sites healed by secondary intention.
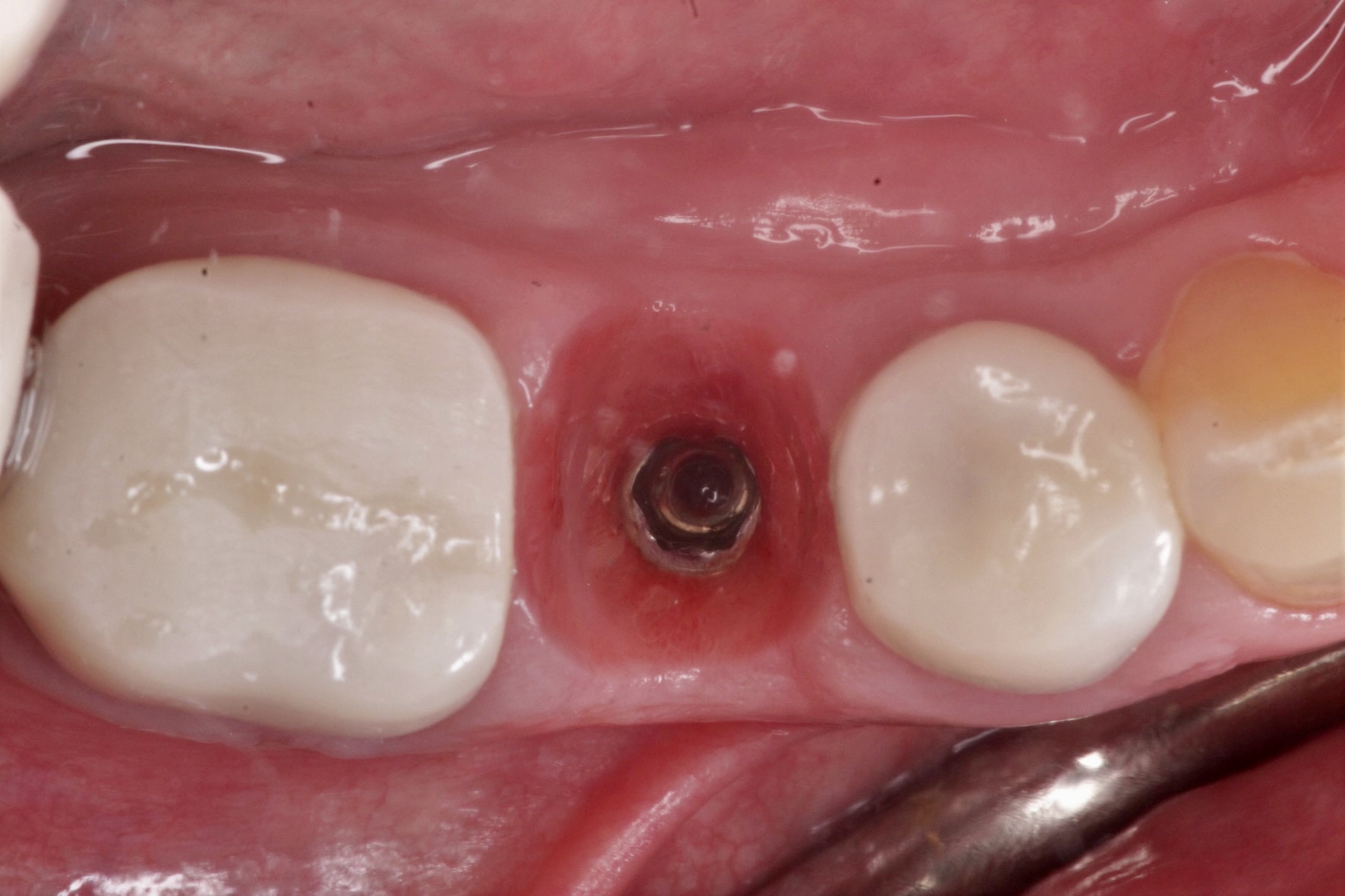
Six weeks post-op the cover screws began showing through the wound
site and the dental implants do not feel as tightly fixated as they were
before. The patient also has one area on his lips where he still does
not have sensation. What should I do at this point? What do you think
of the prognosis?