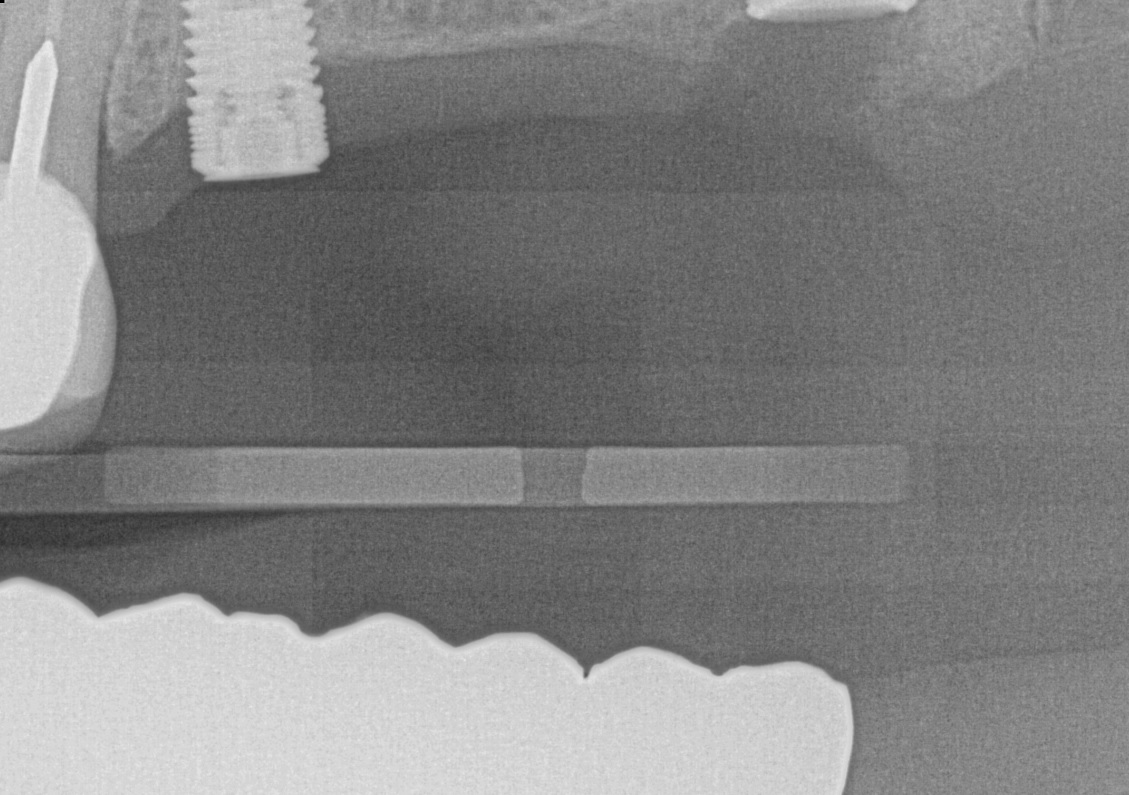
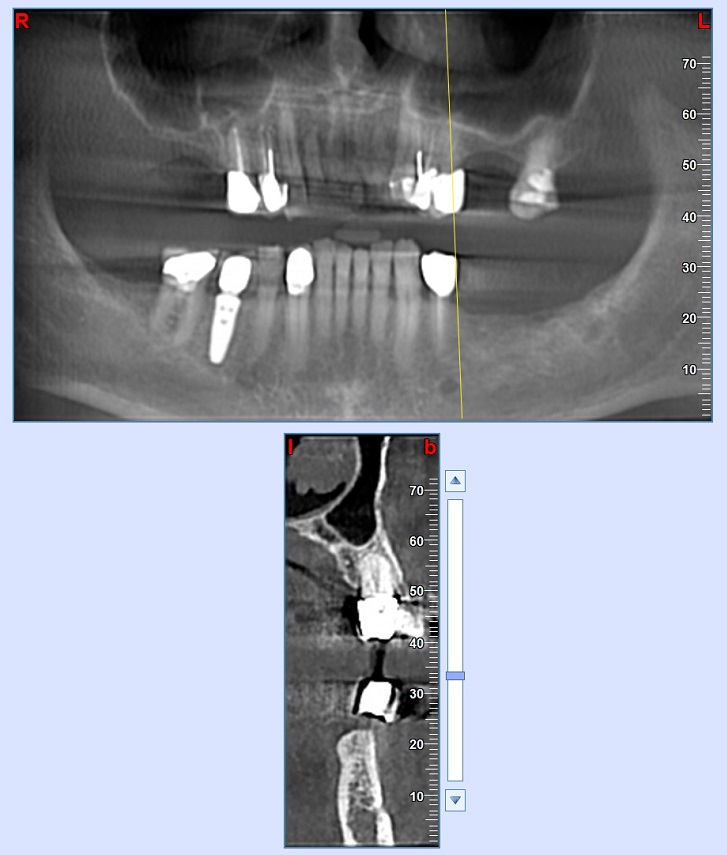
I have a colleague that sent this case for restoration of the two newly placed maxillary implants shown in the attached radiograph. I noticed that the head of implant at No. 13 is exposed through the gum. My question: Can this be predictably corrected with soft and hard tissue augmentation, or would it be best to ask my colleague to consider removal and replacement at the crestal bone level – prior to restoration. Note – the lower opposing will be restored with and implant supported FPD also.
Thank you for your opinions! They are always tremendously appreciated.
Dr. J comments:
Well if you ask about predictability, the answer is no. I would never, not in 1 million years graft what appears to be a very shallow implant placement. It would be great to see a periapical xray but my recommendation at this point would be to remove the implant and place a new fixture in a good prosthetic position.
Guest comments:
Not just great but necessary to see the whole picture😉
A J comments:
Is there something wrong with your eye?
Dennis Flanagan DDS MSc comments:
Have a discussion with the pt. The risks for a perimucositis or periimplantitis, bone loss should be asessed. Allow the pt to make the decision and document evertything. You don't want the pt to come back at you without adequate notes to demonstrate that the clinikcal decision did invilve the pt.
I probably would not soft tisue graft because that would create a deep pocket. The issue of hygiene and a rough implant surface is the issue. You may consider an osseous graft.
A J comments:
Why have a discussion with the patient? The patient's not the one placing an implant there? The patient's not going to tell you how to do your job?
Guest comments:
Probably to avoid a malpractice lawsuit, it’s the patient’s body. Also getting permission from the patient to cover up a poorly placed implant won’t get you off the hook. 😉
A J comments:
Then why ask for permission to get you off the hook?
Bill McFatter comments:
if you restore it you bought the problem You knew or should have known a problem existed and you didn't discuss with the patient before they spent their money on that resotration
Guest comments:
The x-ray posted is inadequate to make a diagnosis there appears to be a another molar implant that is too deep. I’d first repost films that show the entire implants then ask for advice. Don’t understand why preoperative films are included. You could simply send the patient back to the placing dentist for correction. Not your problem.
Guest comments:
What did the placing dentist say about this case? Just curious.
Steingrimur Hermannsson comments:
I had referred this patient to the placing dentist for possible sinus lift and implant placement at site No. 14. However, the placing dentist decided instead to extract and replace 13 and 15 with implants. This is the result we have now. I am concerned about future thread and peri-implantitis without adequate correction. Thank you everyone for your thoughtful advice. Greatly appreciated.
A J comments:
Bingo!! There's the problem right there!!!!???
yup, sinus lift before the implant!?
Guest comments:
I think that you lost control of the case. Both implants seem to be poorly placed and if not resolved now the restorative will be compromised. One implant too shallow the other seems too deep. I'd tell the placing dentist this case is not restorable give the patient a refund and find someone who will work with you. Placing implants at 13,15 is fine to avoid a sinus lift but the two implants are not restorable. There are explantation kits out there. The sites can still be used. When the implants fail you will be thrown under the bus.
Guest comments:
Love OsseoNews , the implant placement “Sports Page”
Richard Winter comments:
Since this is inadequate information to make an informed opinion we can discuss the prosthetic space or CHS. Since the microthreads hold the tissue hemi-desmosomes, it is possible to make an abutment, bone profile the posterior implant and make a prosthesis. You cannot predictably grow bone 360 to cover these threads. You can mill the threads and cover them with your bridge if needed. Best of luck and if there is not adequate CHS, then the implant may require explantation. Again, all theoretical as this is not even close to the information, x-rays, photos, cbct required to make an informed decision.
Timothy Carter comments:
My recommendation would be to restore the implant that the patient paid for and tell them it might not be the most esthetic case but it should provide many years of service. I am glad I am not a patient relying on some of these extremely complicated solutions to simple imperfections that many on here suggest.
Mahijeet Singh Puri comments:
Get the opg done first as there seems to be another implant which is submerged.
Has sinus floor elevation been done also
Let me have a look at the latest opg and then only I can comment
Manosteel Manosteel comments:
Why didn't the placement Dentist place the implant deeper?? Even a sinus lift by hydraulic elevation would work for a 4-5 mm gain. At this point I would look for someone else to place these or learn to do it yourself from Misch or Louis AlFaraje( California Implant institute) . The present implant is useable if it isn't a cosmetic concern and you have min of 10mm of implant in bone. Use an abutment polish any supra gingival implant surface then place a crown or bridge to #15. Don't let a periodontist or OS decide your restorative plan either, if you don't know ,send it to someone who does Prosthodontics.
Greg Kammeyer, DDS, MS comments:
Growing bone around the implant head is possible yet not so predictable. I would inform the patient that it isn't "My best work" and I'd rather redo it ( a recommendation that would stand up to legal scrutiny.) If the patient refuses than flap, grind and polish away the rough surface. This will help keep from having peri-implantitis. Don't restore it "as is".