77 year old male referred for implant replacement of #19. Less than 10 mm vertical dimension between supra-erupted #14 and implant site #19.
Suggestions?
Thanks.
LG
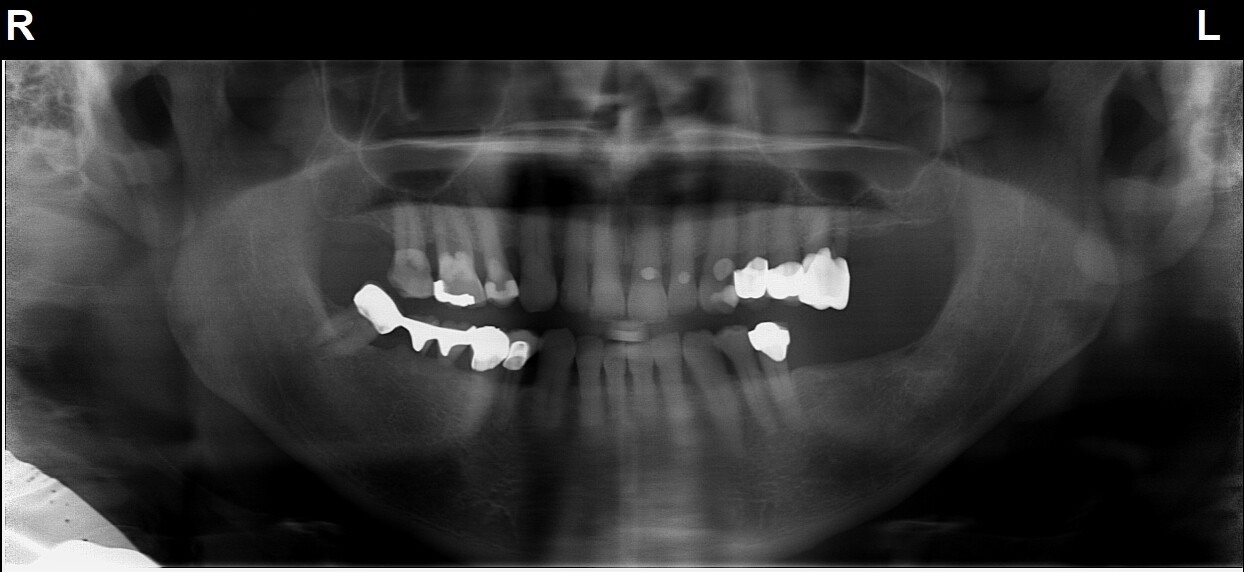
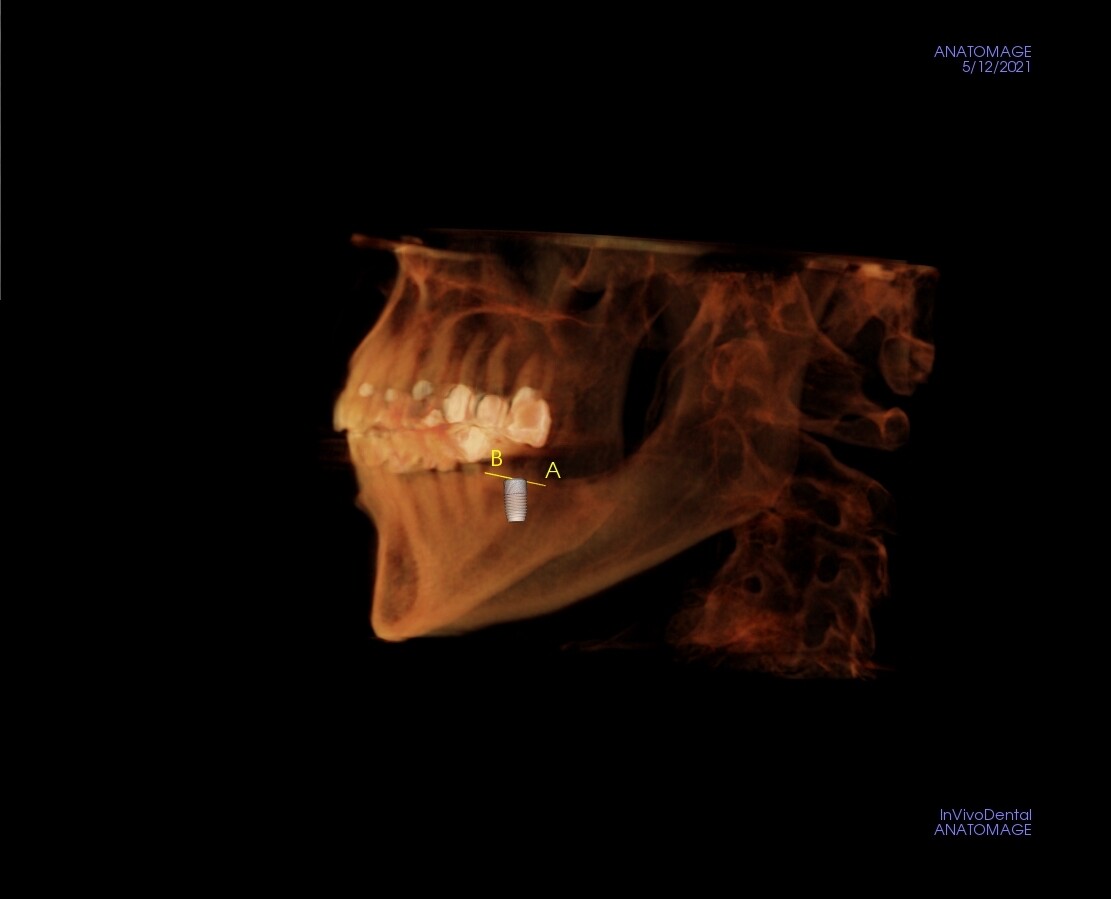
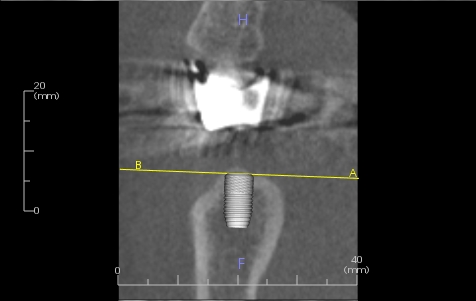

77 year old male referred for implant replacement of #19. Less than 10 mm vertical dimension between supra-erupted #14 and implant site #19.
Suggestions?
Thanks.
LG
Neil Park, DMD comments:
10mm is close for a cemented restoration, but is adequate for a screw-retained crown. Also, if you tell the patient up front that you will be adjusting the opposing tooth, then it is usually accepted by them.hj comments:
Minimum requirement is 5mm for gold crown. It appears you have room for longer implant too.Roj comments:
Theres more than enough room. Why the confusion.Louis Gallia comments:
My question was, there does not seem to be enough vertical height considering the length of handpiece and bur, to place the implant. With the mouth fully opened there is not enough vertical height to fit the handpiece and bur into posiion.Guest comments:
I’m amazed that your placing implants and have no clue on something so basic . Take some basic CE or do a residency and spare your patientGuest comments:
A good clinician would help solve the problem. I think you missed the limited opening issue is very common issue.Guest comments:
The crown on the upper molar should be removed and remade after additional preparation. Not only to facilitate implantation, but more importantly, to correct the plane of occlusion. The pulp is most probably receded enough not to be a problemMahijeet Singh Puri comments:
You are asking 2 different questions 1.not enough space between 14 and 19 2.mouth opening is less for implant drills and hand piece Which one is your problemLouis Gallia comments:
I worded my initial inquiry inadequately. I was referring to the fact that since #14 is supra-erupted, that fact along with limited oral opening does not leave enough room for space needed for collective height of drill and handpiece. Even if I use short drill (13mm). Thanks.Guest comments:
First, you need to address the supra-erupted tooth with a crown, to establish a functional Spee Curve, regardless of limitations in mouth opening. Crown elongation #14, if needed, unless the furcations are a limitation.Guest comments:
I believe the “curve of Spee” is observed on the mandible😉Aldous Wilson comments:
Use an all zirconium or gold screw retained crown. Explain you may need to revisit the issue in future. Next time be more observing, mount the case, or refer out to implantologist.Mihai comments:
Go with the pilot drill, which is shorter. than the second drill0qwl), you can put it from another direction, not just in the ax of 14. Make an insertion path more oblique. After you are with the drill in the hole , you can "verticalize" the path. You negociate the path.Junaid Ahmed comments:
For a 77 year old, he seems to have a more than well functioning dentition. Any medical contraindications? Why was as he referred? Has his ability to function, chew, smile been compromised? Has he requested a replacement or his referring dentist? If there is limited mouth opening, possibly implant placement is then contraindicated. Will save you and your patient a lot of headache! One can place a short implant, for example a Bicon 4.5x6mm implant 2mm subcrestal. At time of restoration, replace the crown on the opposing overerupted molar which will give adequate intraocclusal space for the implant crown.Tim comments:
Plenty of space but no excuse for the incompetency of a so called “implant dentist” asking such questions on a forumGuest comments:
I don’t think you grasped the question. It’s about the limited opening.Guest comments:
Depending on the implant type use an extra short drill to start. Straumann makes a nice set. Also Nobel Active. Once hole is started you can remove your surgical guide and drill to depth with a longer burr. This I find is a very common problem and my presurgical protocol is to measure the opening by trying in my implant handpiece with a short drill in place. 28- 30 mm clearance seems to be the minimum possible due to handpiece size. Problem is if you try to slide the drill sideways you will get an oval osteotomy which can compromise the initial stabilization and the implant won’t integrate. Always bury these cases and allow to heal 2nd stage uncover. This is a common problem, I got burned a couple of times. Also consider restoring the supraerupted #14 to gain a few millimeters, Not all patients can open 40 mm!PAUHA comments:
somehow make an initial osteotomy, once drill is few millimeters inside the bone, u will have more space for vertical movement , second, remove upper crown or grind, as much as possible to gain more vertical spaceGuest DMD comments:
Your first mistake is that, from a functional standpoint, you're only seeing one implant and not the whole picture. Moreover, if you can't solve a simple problem like mouth opening and, if you don't see that the #14 needs to be re-restored in order to restore the occlusal plane's Spee curve (for proper mastication) you need to refer this case out. You clearly don't have the necessary experience and need MUCH MORE training! Do yourself, AND the patient, a favor and refer him to an OS. Asking such questions on a forum on a simple case like this smacks of incompetence. You should not even attempt this case. You're nowhere near being ready. Get some serious training!