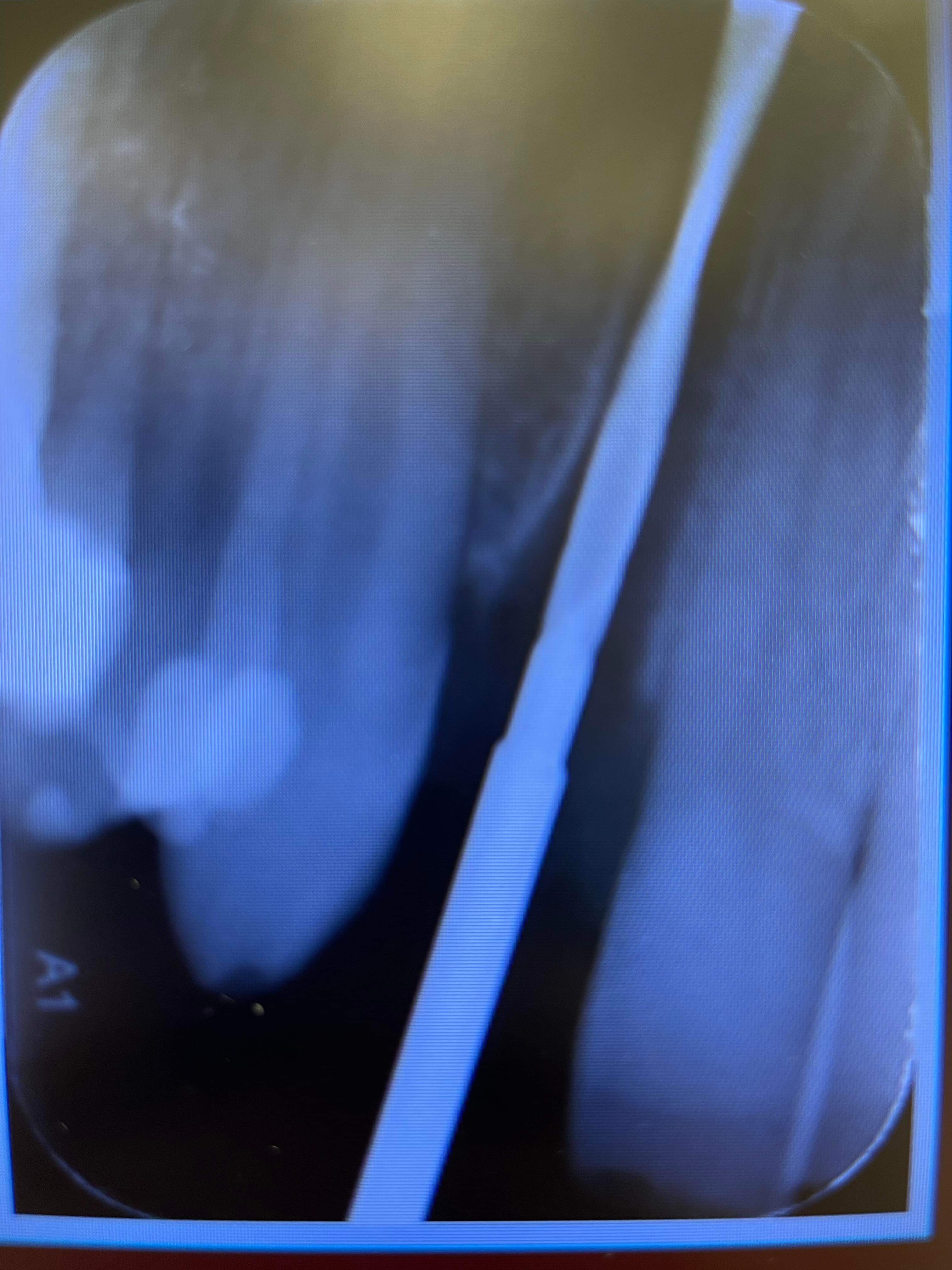
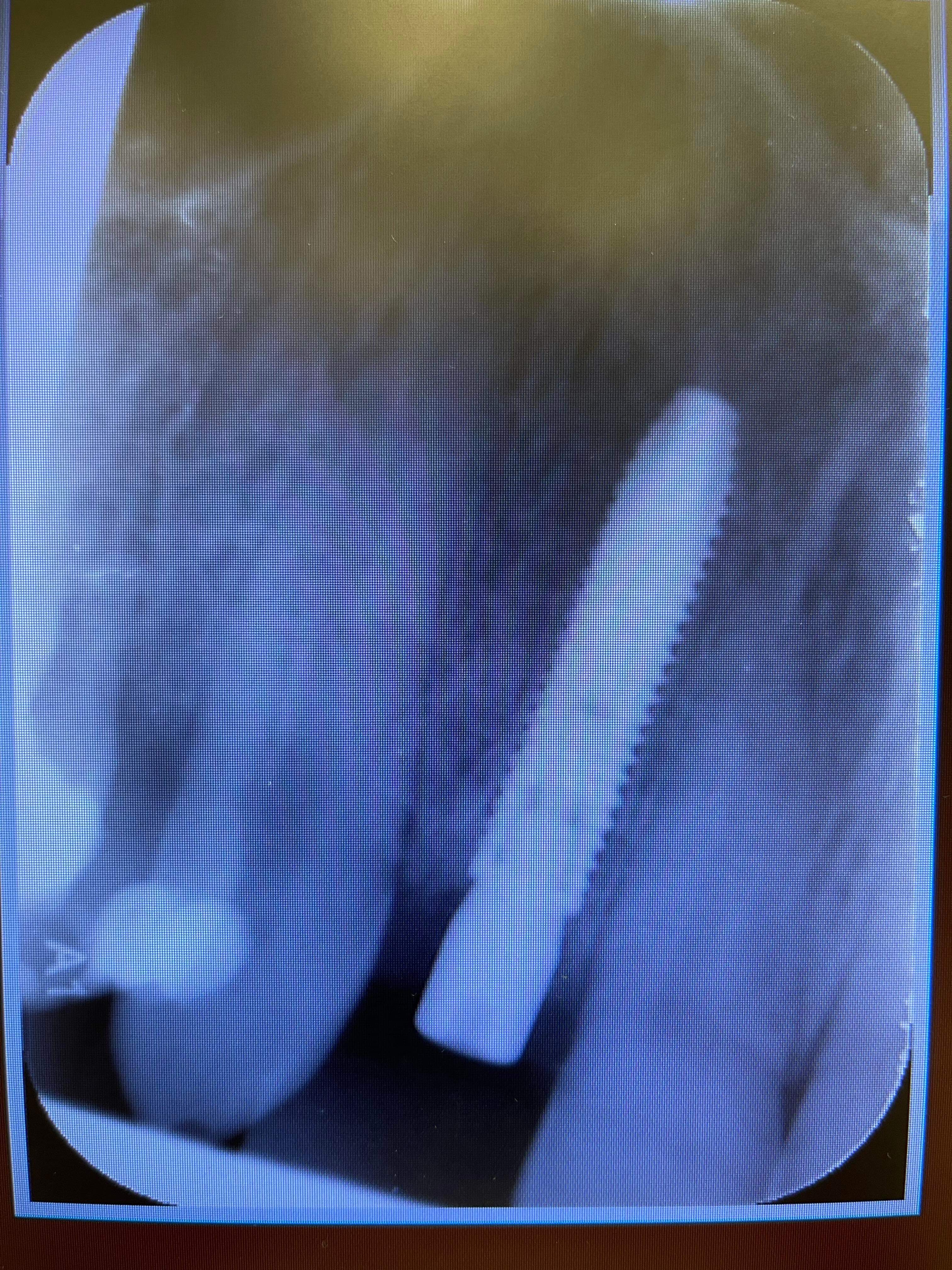
Implant was placed aprox 4 weeks ago after extracting tooth because of periapical reaction and multiple decementations of stift plus crown. I checked the angulation of the root of the tooth, took also control picture(2.0) and still end up in not so favorable distance until 1.1(maybe bad fixture(3.75),should have picked a 3.0). Patient was and is asymptomatic. I took a control picture 4 weeks after and the outcome. Patient also is telling me that he is waking up in the night with clinching teeth and also is smoking. I also noticed the rapid papilla and bone loss mesial. I will explant the implant ASAP and graft the alveolar. What would you do? Tooth 1.1 is positive to temperature,negative to percussion.I am looking for honest opinions and help from surgeons or doctors who had or treat similar situations.Thanks


Tim comments:
I think the problem is that the adjacent tooth is finally becoming symptomatic from the trauma and has had all it can take. Endo #8 unrelated to your implant treatment and there is nothing wrong with your placement or choice of fixture. As far as the "rapid bone loss" I think you are being too critical of yourself as the bone is at top of the fixture, exactly where it should be after 1 month of transmucosal exposure. Treat the adjacent tooth and drive on.Anonymous Anonymous comments:
Hei Tim:) thanks for response.You suggest that the translucency is because of 8?And i should treat endodonticaly and monitorize the evolution?I also did percusion on implant is negative…Tim comments:
If I read your post correctly you said # 8 is symptomatic and the implant is stable. Whatever trauma caused #7 to need endo/post/core/crown most likely affected # 8 as well. It is possible that enough is finally enough and it went south. There may very well be a problem with the implant and it could still fail but I would not blame it on your choice of 3.75 vs 3.0 platform.Anonymous Anonymous comments:
Yes maybe i did not express myself well,i did a test for vitality of 8 and it was positive.I just want to learn from others that have maybe more experience that me.And of course take the best decision for the pacient regarding future treatment.Thanks for taking your time responding.I was thinking that its just 4 weeks after placement of implant so i need to act ASAP,limit the damage.But i want to be sure i do the right thing.20yrsimplanting comments:
its likely that there was residual bacteria when implant was placed leading to implant contamination and abscess formation. explant, clean out and wait a few weeks for body to clear area then go in again. it can happen with immediate placement its not related to immediate loadingTim comments:
In the absence of crestal loss around the fixture I don't think you are wrong to leave it. This may not go over well on this forum but simply accessing the apex of the fixture as if to do an apico and debriding could work as well. Bottom line is that the implant is stable, there is no evidence of crestal loss and the area had a compromised endo to begin with. IMHO you could make this as big or little of a problem as you desire but removing the fixture now could further complicate the outcome because crestal loss is inevitable if you do.Anonymous Anonymous comments:
🙏I have time until next week to think,hope i can sleep.Even if i place a lot of implants,some times i feel that i f…up and that is afecting me so bad.I found out that talking to others(doctors,experienced) helps me.Thanks again🙏Guest comments:
An implant with that kind of periapical lesion is not stable. Crestal bone level is not the only factor for succes or decision making. Accessing the apical area might be an option when we have a fully integrated implant, however here it is only 4 weeks, so explant is better.Anonymous Anonymous comments:
I plan to explant it ,hope is not that stable and i can torque back:(.ThanksTim comments:
That would be safe and clearly nothing wrong with that approach. In the absence of mobility of the implant I would be inclined to treat the radiolucency via debridement without a graft material and endo 8. I believe that if the fixture were the actual cause there would be mobility and radiographic evidence of soft tissue attachment extending from the crest (even at only 4 weeks). This is just my opinion and unlike Matt Helm I will not criticize anyone for disagreeing and removing the fixture. The fixture may indeed fail but after 20 years of doing this I have learned to treat these things a little more like the teeth they are designed to replace. Thanks for posting and for your honesty.... a lot of people would try to blame "Another Office" that placed the implant!!Anonymous Anonymous comments:
Thanks Tim,i will sleep on it(hope i use this sentence corectly)and take a decision.Have to solve my problemes and try to not repeat them as much as i can.Wish you a great weekend.Guest comments:
The implant has a huge periapical lesion that is causing the symptoms. Remove the implant, do a thorough curettage of the lesion (no grafting here with the infection) and prescribe systemic antibiotics. Monitor 11 to see if an endodontic treatment is necessary in the future. In general, I think you asked a little bit too much from nature… immediate implant with immediate loading in an endodontic compromised site in a patient that smokes and clenches… better to take your time and do everything one step at a time.Anonymous Anonymous comments:
Thanks,i admit that i did not checked the chiped incisal edges of the other teeth(bruxism) and pacient related to me about it 2 weeks after implant placement.I decided to make a oclussion gutiere ,but to late.Bad jugement overal.Dr Kambiz comments:
The fact is you have a apical infection at 1.2 according to X-ray progression. The vitality of 1.1 is also questionable. To play it safe, I would remove the implant and do curettage the infection, then wait 6 weeks for infection to clear. During this time I would watch and test further the 1.1 and do endo if indicated. Then replace the implant again and BURY it please for 3 months.(don’t worry you ont get much of a resorption after 6 weeks, like someone suggested here) There is too much hype and patient pressure when it comes to immediate anything, while the actual indication is probably only 1 in 100. This was clearly contraindicated in my books. Many would disagree with me, which is fine , but my painfully learned lessons and common sense, are something I cannot ignore.Anonymous Anonymous comments:
Thanks Dr G,i would be more selective with my cases after this.I was thinking to explant ,wait 3-4 months.(meanwhile make a Maryland bridge or Peek structure) then place a new implant .I also thought of placing some bone after explantation of implant but after reading opinions (better not due to active process).Richard Waghalter, DDS comments:
Dear AA, I am in agreement with some of your hindsight. However, you did not explain why you had to extract the tooth. Was there any soft expansion of the external apical mucosa? If the patient bruxes or has a slide in centric, the tooth up front gets the trauma until the slide in the occlusion is corrected. The crown in question does not fit the tooth well. Was there any mobility or fremitus in CO or was it the whole tooth? There appears to be adequate bone support. Another explanation of the less density of the apical portion of that lateral incisor can be that the apical portion of the root poked through the alveolar bone due to positioning and/or the labial bone being very convex in shape in that area. The soft tissue was traumatized by the bur. As for the radioluency around the implant: it could be that excessive pressure or 'burning' of the bone from inadequate cooling irrigation during the time of placement.The damage to the bone and the fact that the implant extends past the apex of the central are related. The close proximity of the implant and root end probably revitalized the central. Be sure to reduce the implant and the central until they are within the confines of the bony housing. Do an occlusal analysis and bite adjustment before placing the abutment and crown on the lateral incisor implant before impressing for the new crown. And, evaluate the bite after the final restoration is placed. Finally, evaluate the patient for sleep apnea. I appreciate the fact that you were amenable to problem solving through peer review.Anonymous Anonymous comments:
Dr.Richard thanks for opinion:The osteotomie was in to the palatal wall,implant is completely into bone walls.(I have also a cbct that I took recently,strange that the black area is from what I see just around implant).Tooth 1.1 is reacting to cold stimul,perhaps still vital?.I intend to explant the implant(even tho is asimptomatisk to lateral ,axial percussion).True pacient relatates that he wakes up in night with his teeth closed(bitting).The theory of bone heating can be….I admit to like using some buts without water,low speed to take some autogeneous bone.Bottom line plan is to explant,let it heal 4 months,then place a new one but burried.Any other idea?Also check 1.1Anonymous Anonymous comments:
Tooth was extracted because of root fractures,old endodobtic treatment that had also chronic apical periodontitis.Greg Kammeyer, DDS, MS comments:
Either you awoke a sleeping dead tooth at #8 or more likely didn't clean the small apical lesion adequately on #7. I recommend whenever you treat a site w prior RCT that you use a dental curette and then #8 round burr aggressively in any area you question, to remove any diseased tissue. Since #8 is testing vital, I would remove the implant, clean the lesion aggressively, flapping buccally enough to get buccal access, graft and then wait 4 months. Re-eval the vitality of #8 at 2 months, and take a post op radiograph after the graft to confirm the space is filled. Good luck!!