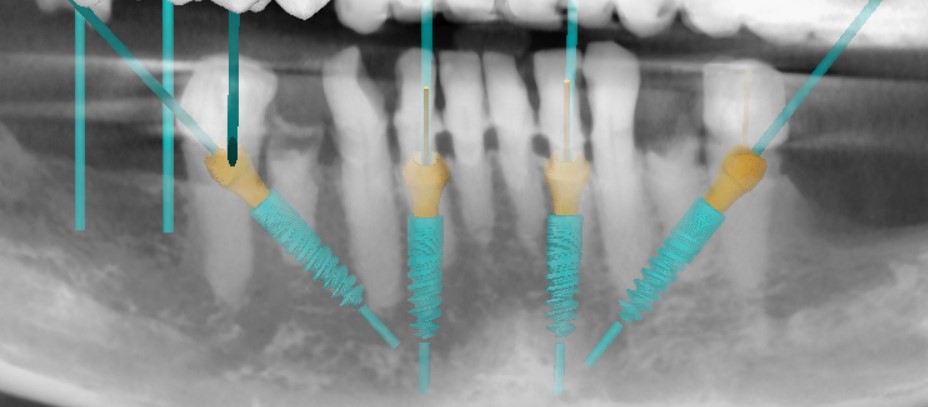
Hello I just met a patient for full arch lower reconstruction with implant-supported fixed teeth. Remaining teeth : LR5 to LL5, knife edge ridge posteriorly. Most distal position for implant placement is between LR4-5 and LL4-5. So, in order to extend the A-P spread I want to tilt distal implants. Still, the mental foramen is just under the drilling site, so I am considering tilting the distal implants for 45 degrees. Never done that before (45 degrees tilting). What is your opinion regarding: 1. cortical bone stress distally of the distal implant? 2. what about the implant-MUA interface mechanical stress distally? (I use morse tapered implants) Thank you for you time.
Dr T comments:
I see this done every day..Dennis Flanagan DDS MSc comments:
Need CBCT but 2.5X10,11,5 may work, control occlusal loadingFrank comments:
First, you will have to make more reduction of the crest to allow prosthetic space. Why not plan 30 degrees as most angled abutments are 30 degrees. I don’t see that you will add that much AP by going 45. In fact on the scan cut you show us, you are close to 30.Aquiles comments:
I agree. This case is not too complicated. Slices of the mandible would be nice to evaluate thickness. Taking down the ridge is important to give you width. And tilting more than 30 degrees will cause you trouble when you go to restore the case. You would possibly need full custom stuff from someone like true abut or something like that. You want to avoid bespoke parts in my opinion. Why add the expense. And also the results would not be necessarily better with 45 degree angling. Be sure you have restorative specs for all your parts before anything. I’d do a digital surgery first and plan all your steps ahead.Dr. Michael T comments:
Thank you for the response.1. Taking down the ridge doesn't give me width since these would be immediate implant placements. The wider part of the ridge is just the coronal part of it. Still, I have to cut down a bit to get more prosthetic space and even ridge morphology.2. Restoration is not a problem, since as you can see at the X-ray I have 45 degrees MUAs3. I attach a pic with both 30 and 45 degrees tilted implants. My gain is 3-4 mm each side, almost half a premolar. I would like to get that small increase at AP spread provided that 45 degrees wouldn't jeopardise the final outcome.So, my question still not answered.Would the 45 tilted implants have a negative impact both biologically (bone interface) and mechanically (abutment-implant interface)?Thank you for your time.Tim Carter comments:
I think you need to answer the most important question which is "Why are you removing these teeth and what about the maxilla"?? If you offer traditional periodontal therapy then your question is irrelevant.Tim Carter comments:
I think you are opting to kill a fly with a hammer. This is not a difficult case and there is no rational reason to limit your restoration to a 4 implant cookie cutter protocol plan. Just because Nobel Biocare marketed All on 4 with angled distal fixtures does not mandate that as "The Cure". Consider 5 or 6 fixtures with shorter ones distal or better yet Periodontal therapy with conventional fixed... believe it or not that type of actual dentistry is still possible and not every patient needs to suffer from titanium deficiency.Dr. Michael T comments:
Thank you Dr. Carter. It’s always good thinking out of the box. I re-considered my plan and I am now thinking of restoring on top of the existing lower teeth. The main reason is that A-P would be bigger restoring the existing teeth. Just a few things to point out. 1. I am not an All on four fan. Actually I don’t like and always place 6 implants. Still this is not a 6 fixture case. The bone width distal to 5s is 1 mm max. 2. Implants are not more profitable for me, since a charge a fixed fee for for arch lower restoration, whatever it is. 3. What makes you think I am not treating the upper as well?Thank u for your advice.
timcarter comments:
I assumed you had no intention of treating the maxilla because you never made any mention of it. You still haven't made any mention of the periodontal status of theses teeth and why you would opt to remove them... I see this case as one that could benefit from more traditional dentistry and you have made no mention of anything other than more implants.Tim Carter comments:
Please justify the need to extract these teeth in the first place and why would you treat the mandible as such and ignore the maxilla. I would hope that periodontal therapy of some sort is planned for the upper arch if/when you create a case study out of this lower arch and my 20+ years of experience would suggest that the lower arch could benefit equally from perio therapy. Obviously treating this a case of insufficient titanium is likely more profitable for you but likely not in the patient's best interest.