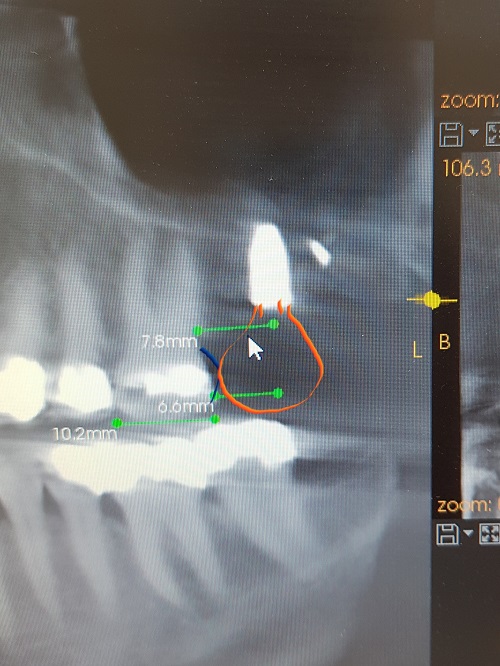
This is my 2nd implant case. Implant was placed in the upper left 2nd molar position with internal sinus lift. After the operation, with control x-ray, I found out that the implant is quite distally positioned. The distance between buccodistal root of 1st molar and mesial aspect of the implant seems to be 5 mm at least. I am quite concerned about the prosthetic prognosis in this way, due to mesial cantilever effect of implant crown and food stuck in the future.
I have deeply considered about either removing the implant out and positioning more mesially again or as a compromise adding some composite resin on distal surface 1st molar, approximately 2mm thickness with anatomical shape and making crown on the implant.
The used implant is Nobel Biocare, cc parallel with size of 4.3 × 8.5. The primary stability was 15 N. The operation has been done a day before this case post.
I would like to get some advices on this issue from others that my have more experience.
Thank you.
mark comments:
leave it alone. what is that opaque fragment distal to it?
next time plan better
Lavish Peanut comments:
Okay. That is debris of root canal filling from extracted 16. After I extracted 16, I could see its orange color of gutta-percha, and I couldn't take it out. Also was afraid of perforation.
drgilani comments:
Crown would be fine, it seems. 15 Ncm is too little. you should go to 30 Ncm minimum for primary stability.
That little fragment is a micro UFO, never mind.
Lavish Peanut comments:
Thanks for the reply.
How do you evaluate survival rate/prognosis of the implant with weak primary stability compared to stronger one?
15 Ncm would compromise osseointegration in this case?
I am planning to wait minimum 6 months, due to weak stability and internal sinus lift with bone graft.
peter.hunt@drpeterhunt.co comments:
This happens all too easily with free-hand placement. It's hard to get the implant drills around the back of the upper molars and the natural tendency is to go further back.
You should be fine here though. You have the implant nicely vertical and in a reasonable depth of bone. For a second implant, it’s very gutsy!
Let it heal, see how it survives then you can work out the restorative options. Your idea of adding to the distal of the first molar seem entirely reasonable, though this might be easier done by placing a crown.
Lavish Peanut comments:
Thanks for the reply.
Yes exactly. I was quite struggling with obtaining proper view and measuring distance.
I would leave it then. Also other colleauges mentioned a crown would be better.
Just bit hard to bring 14 to be crowned because it’s vital with some filling on it and crowning was not in the plan. But as you said, I will wait for the survival first.
jyothi.charlie@emiratesho comments:
You can change the filling on the first molar with a ceramic onlay which has a good contact with the crown on the implant.
Do it when you take the measurements for the crown, and the Lab can do a good contact ,
This will be less invasive than a crown on the first molar.
Lavish Peanut comments:
That could be a good solution as well. I will consider it, thank you :)
JeffT comments:
Just curious- was this patient having mastication problems with 1st molar (+) occlusion?
Lavish Peanut comments:
I am sorry, but (+) occlusion here means cross bite or the bite is high on 1st molar?
JeffT comments:
Sorry for the confusion. I was indicating that the maxillary first molar is occluding a little with the mandibular second molar. So your patient has slightly more than first molar occlusion (which for the vast majority of patients is plenty; see the literature on SDA or shortened dental arch). I would really hesitate to do so much treatment in this situation.
Best regards
Matt Helm DDS comments:
You should be fine. Since you're planning to let it heal for 6 months the low primary stability should not be an issue, but do check it prior to restoring! The best solution is a crown on the first molar, BUT, IF there is sufficient coronal structure then an onlay is much more elegant and much less invasive.
Lavish Peanut comments:
Thanks for the reply and advice! :)
GregKammeyer comments:
I'd leave it. You should get more training about working around the sinus. Retrieval of the foreign object isn't harder than an SA2.
Lavish Peanut comments:
Which instrument or technique could be used to take out that foreign object stuck at apex near the sinus?
After the extraction of 16, I could see it through palatal socket. And tried to loosen it with tip of thin explorer for 10~15 minutes. It did not move at all.
I was considering about using thin root picker, but eventually it did not fit into the apical part of the socket.