Dental Implant Perforation
Dr. Steinberg asks:
I just started placing dental implants. I took courses for 5 years before I felt confident to place an dental implant on my own. The only area I feel I really need to master is using CT scans for treatment planning since I had the following disaster.
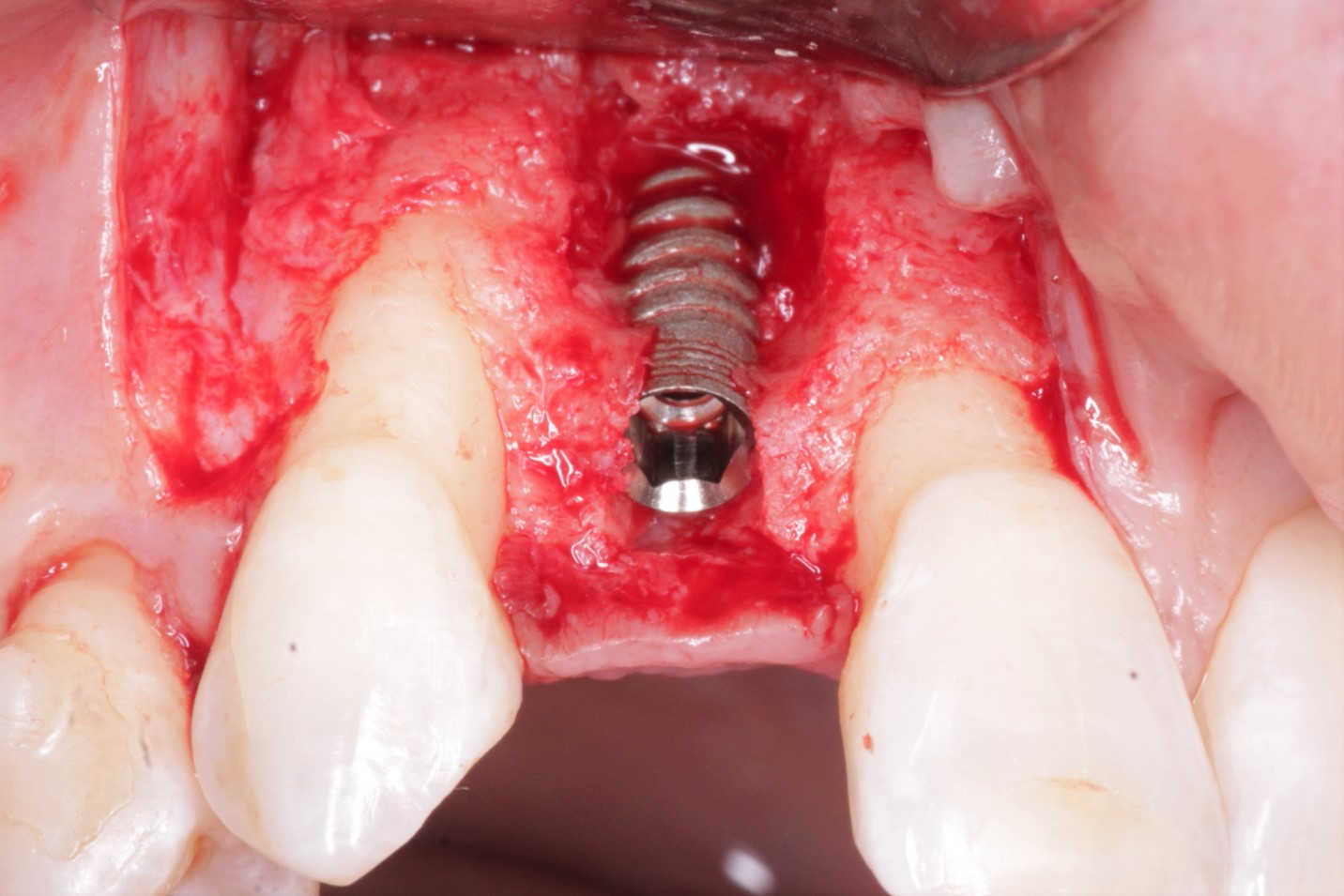
Here is what happened: I was placing a dental implant in the maxillary lateral incisor position and I perforated through the buccal cortical plate when I torqued down the dental implant. I thought about placing a mineralized freeze dried bone graft and repositioning the flap. But I panicked and sent my patient over to the oral surgeon. Did I do the right thing? What would you have done? Thanks for any comments.