Compromised Implant Case: Design Options for to Avoid Failure?
Last Updated: Mar 27, 2019
I agreed to see a patient that another family was helping out. Patient fell on hard times and his mouth had many serious problems. I agreed to do comprehensive implant dentistry on the patient, used high quality lab for treatment planning, surgical guides and immediate temps. At the time, 72 yr. old male, had knee replacement in 2010, arthritis, HTN controlled with medications and NKDA. Upper was planned All-on-5, lower All-on-6. Patient first came to see me at the end of 2017. In March 2018, I extracted remaining teeth, performed guided bone reduction, guided implant placement and guided immediate PMMA reinforced with bar screw-retained temps for upper and lower. The lab representative was present at time of surgery and had my own lab technician refine the temps while I closed the case.
Surgery and immediate restoration went smoothly, no complications, all performed under local anesthesia only. Pt. started on Amoxicillin 2 days prior to appointment and took for 10 days total. I gave Decadron starting day of surgery for two days and Vicodin/Advil PRN. Pt. had no post-op complications in terms of infection and pain was controlled with Advil, and only took Vicodin day/night of surgery. Immediately discovered at surgical appointment, that patient was in an anterior open bite with his temps. Adjusted occlusion until pt. had group function, but he did not have anterior guidance. I gave pt. POI, soft food diet and normal follow-up appointments. (See photos below of pre-treatment and CBCT slices of immediately after placement and restoration with PMMA temps).
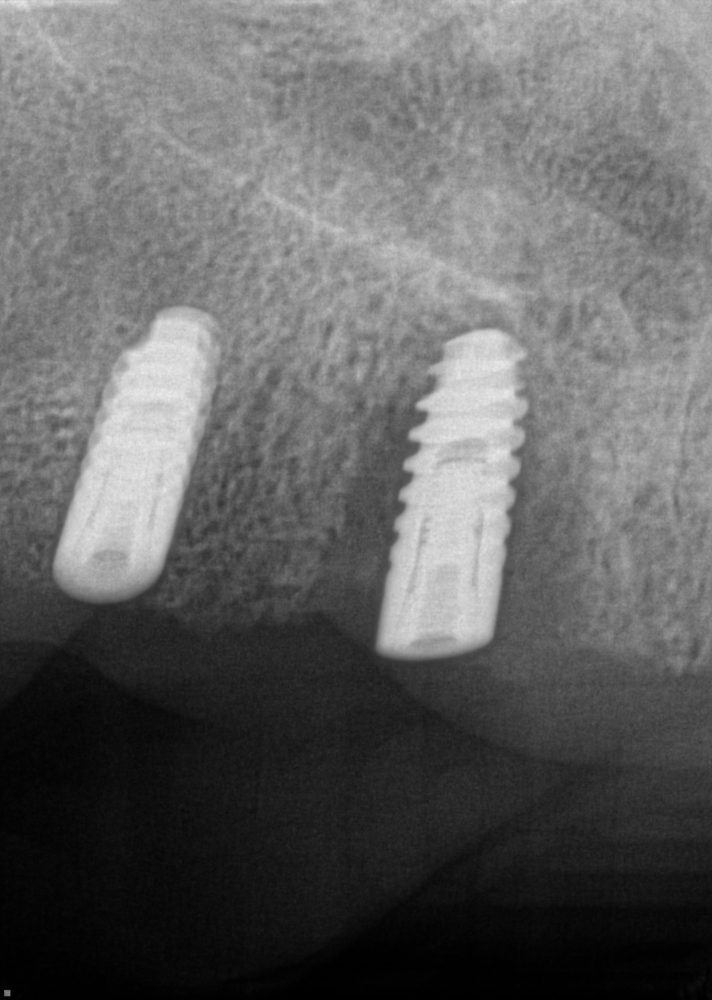
After weekly checks on occlusion, 2 months after surgery, the upper right side was painful to patient and it was noted that it was moving/loose. I removed the prosthesis and found that all implants were loose and needed to be removed. #30 was also lost. Made denture, removed implants and let area heal. In November of 2018, we performed surgery on the maxilla, placing 5 short implants in #4, 6, 9. 10 and 12 sites. (See x-rays included). I buried implants and had pt. continue to wear upper denture. 6 weeks later, took periapical x-rays and #8 failing implant and was removed.
Now, all implants were integrated and stable, we are ready to restore. Lower is easy, screw-retained hybrid or Zirconia bridge is planned. The upper is where I am having a little trouble treatment planning. My undergrad degree is biomedical engineering and I understand about stress/strain/force on implants and surrounding bone along with material properties. However, I am scared after the failing implant experience on the upper. So my options for the upper are as follows: Tissue supported, implant retained option of 4 Locator attachments and an upper horseshoe with metal palate denture. Or Implant supported, implant retained options of upper bar with Hader clips and Locators with hybrid horseshoe denture or upper Panthera bar and hybrid prosthesis or screw-retained hybrid prosthesis. I’m leaning towards the upper bar with Hader clips and Locators for best support during function, and splinting implants. I’m just nervous about #4. If that implant fails, pt. loses bar and then is converted to Locators and only on the left side. Anyone have any thoughts on what is best long-term solution to help #4 avoid failure?

![])](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2019/03/19682-24-8-failure-c9b72123c1da-e1553691843773.jpg)Failure
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2019/03/19682-24-cbct-after-1st-srugery-upper-c9b72123c1da-e1553691908160.jpg)CBCT After 1st Surgery Upper
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2019/03/19682-24-cbct-after-1st-surgery-lower-c9b72123c1da.jpg)CBCT After 1st Surgery Lower
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2019/03/19682-24-cbct-after-1st-surgery-c9b72123c1da-e1553691964180.jpg)CBCT After 1st Surgery
![]](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2019/03/19682-24-cbct-after-2nd-surgery-c9b72123c1da-e1553691994523.jpg)CBCT After 2nd Surgery
Failure){kind=link}
CBCT){kind=link}
CBCT){kind=link}
CBCT){kind=link}
CBCT){kind=link}
21 Comments on Compromised Implant Case: Design Options for to Avoid Failure?
Dennis Flanagan DDS MSc
03/27/2019
Eric
03/27/2019
Dennis Flanagan DDS MSc
03/27/2019
Dennis Flanagan DDS MSc
03/27/2019
Joseph Kim, DDS, JD
03/27/2019
Richard Hughes DDS
03/27/2019
Dok
03/27/2019
Dr Dale Gerke, BDS, BScDe
03/27/2019
Eric
03/28/2019
Ed Dergosits
03/28/2019
Ed Dergosits
03/28/2019
Eric
03/28/2019
Eric
03/28/2019
Eric
03/28/2019
Greg Kammeyer, DDS, MS, D
03/28/2019
Eric
03/28/2019
Matt Helm DDS
03/29/2019
Riyaz K Gangji DDS AFAAID
03/28/2019
Eric
03/28/2019
Matt Helm DDS
03/29/2019
Featured Products
Classic 50/50 Mix
Promotes osteoconduction
Provides structural integrity
Convenient Syringe!
50/50 Cortical/Cancellous
Available in 3 sizes.
Eliminate hassle of mixing particulate grafts
Sold in packs of 5 or packs of 10.
Proven safe, and clinically effective
Resorbable collagen membrane derived from purified porcine pericardium
Fast hydration and excellent tensile strength
Good adaptation to various defects
Excellent tear function and duration
100% allograft
Eliminates mixing hassle
Moldable after hydration
Richard
03/27/2019