Bone Graft with Implant Placement: What option do you recommend?
Last Updated: Oct 04, 2018
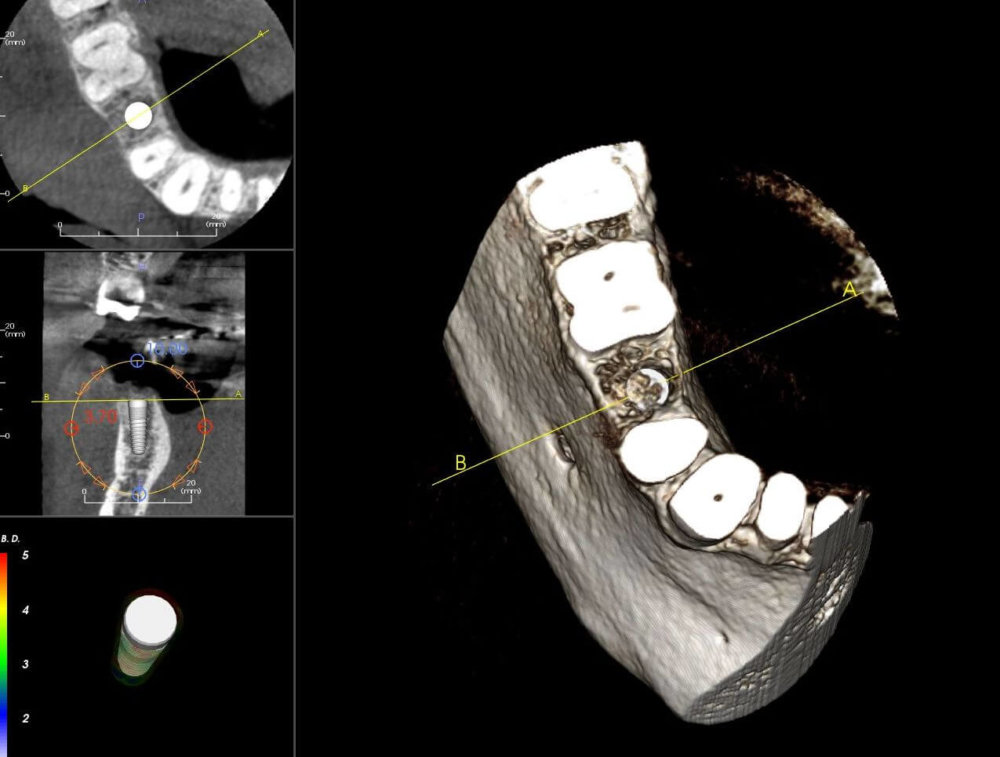
This graft at site #29 has been in place for 6 months. The bone is generally good except for some gaps notably around the lingual aspect. Both lateral plates are intact.
Here are the Options: 1) placing implant as is 2) placing implant with bone graft to fill gaps 3) redo graft and wait.
What option do you recommend?
![]Bone Graft with Implant Placement](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2018/10/8162-24-1-bb56c1c424b8-e1538658077386.jpg)
![]bone is generally good except for some gaps notably around the lingual aspect.](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2018/10/8162-24-2-bb56c1c424b8-e1538658030493.jpg)
{kind=link}
{kind=link}
5 Comments on Bone Graft with Implant Placement: What option do you recommend?
Osurg
10/04/2018
Timothy Hacker DDS FAAID
10/04/2018
Sdddds
10/04/2018
BJP DDS DICOI
10/04/2018
Featured Products
Classic 50/50 Mix
Promotes osteoconduction
Provides structural integrity
Convenient Syringe!
50/50 Cortical/Cancellous
Available in 3 sizes.
Eliminate hassle of mixing particulate grafts
Sold in packs of 5 or packs of 10.
Proven safe, and clinically effective
Resorbable collagen membrane derived from purified porcine pericardium
Fast hydration and excellent tensile strength
Good adaptation to various defects
Excellent tear function and duration
100% allograft
Eliminates mixing hassle
Moldable after hydration
Timothy C Carter
10/04/2018