Complex Medical History: Should I Proceed with Implant Treatment?
Last Updated: Mar 19, 2016
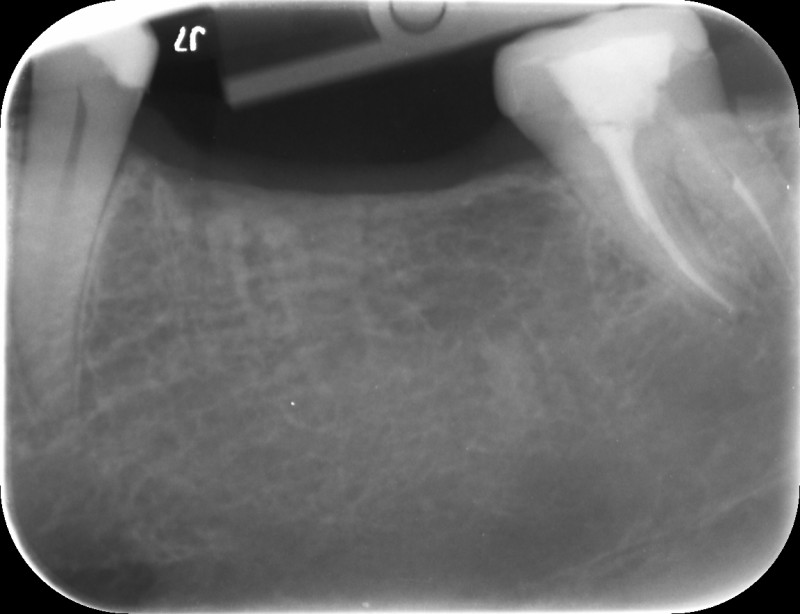
This 39-year old male patient would like implants to replace #18, 19 and 30. Clinically and radiographically there appears to be sufficient bone (see attached x-rays). The problem is that he has a complicated medical history.
He has suffered avascular necrosis of both hips requiring hip replacements. This was caused by pancreatitis, as a result of alcoholism. He is now off alcohol.
His daily medication includes ciraplex 10mg, gabapentin 600 mg, oxycodone 15mg, klonopin 0.5mg-2mg,morphine sulphate 60 mg,omeprazole 40 mg, simvastatin 20 mg, multivitamin and fish oil
It appears like a great case to do surgically but I’m concerned about his medical history.
Any thoughts whether I should provide treatment?



19 Comments on Complex Medical History: Should I Proceed with Implant Treatment?
CRS
03/20/2016
LDRN
03/31/2016
Alex Zavyalov
03/22/2016
Jawdoc
03/22/2016
DrT
03/22/2016
Dennis Flanagan DDS MSc
03/22/2016
sergio
03/24/2016
Dr. Gerald Rudick
03/22/2016
Jack Yetiv, MD. PhD, JD
03/22/2016
LSDDDS
03/22/2016
kent hamilton
03/22/2016
Dr. Vipul G Shukla
03/22/2016
The other Dr.T
03/23/2016
vijaykumar bokkasam
03/23/2016
Roxanne
03/26/2016
CRS
03/28/2016
Roxanne
03/30/2016
broach1
04/05/2016
Featured Products
Classic 50/50 Mix
Promotes osteoconduction
Provides structural integrity
Convenient Syringe!
50/50 Cortical/Cancellous
Available in 3 sizes.
Eliminate hassle of mixing particulate grafts
Sold in packs of 5 or packs of 10.
Proven safe, and clinically effective
Resorbable collagen membrane derived from purified porcine pericardium
Fast hydration and excellent tensile strength
Good adaptation to various defects
Excellent tear function and duration
100% allograft
Eliminates mixing hassle
Moldable after hydration
Jawdoc
03/20/2016