Failing implants after loading: Why is this Occurring?
Last Updated: Jul 24, 2012
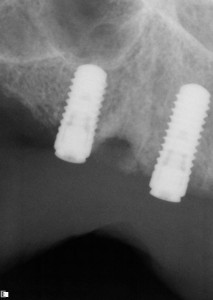
In December 2011, I placed 4 dental implants in the maxilla of a 60 year old healthy male patient. 3 implants were ITI bone levels and 1 was Blue Sky Bio tissue level. Below are the films. The implants appeared integrated. They were uncovered, healing abutments placed and later locator attachments were picked up in his provisional full coveraged denture. The implant in the 6 position showed signs of failure. The problem is that now the 3-4 position implant is also loosing bone, although it is asymptomatic. I removed the locators and asked the patient to use adhesive as needed till I can uncover the new implant. However I am quite concerned as to why this is occurring? (the denture fits well with decent occlusion). Any thoughts or comments are welcome.
(click images to enlarge)
![]failing implants after loading: post insertion](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2012/07/nar1.jpg)post insertion
![]failing implants after loading: left side](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2012/07/nar212.jpg)left side post insertion
![]failing implants after loading: february](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2012/07/nar2121.jpg)failing prior to problems in feb 12
![]failing implants after loading: april](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2012/07/nar412.jpg)failing implant in april
![]failing implants after loading: 3/4 position](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2012/07/nar612.jpg)other implant in 3/4 position, note new implant in 7 spot
{kind=link}
post){kind=link}
{kind=link}
left){kind=link}
{kind=link}
failing){kind=link}
{kind=link}
failing){kind=link}
{kind=link}
other){kind=link}
40 Comments on Failing implants after loading: Why is this Occurring?
gary weider
07/25/2012
Baker k. Vinci
07/26/2012
Michael
07/24/2012
gary weider
07/25/2012
Theodore Grossman DMD
07/24/2012
gary weider
07/25/2012
Alejandro Berg
07/24/2012
DrT
07/24/2012
gary weider
07/25/2012
Greg Steiner
07/26/2012
Carlo Maria Bolognesi
07/24/2012
Gregori M. Kurtzman, DDS,
07/24/2012
gary weider
07/25/2012
BARROW MARKS, DDS
07/24/2012
dr. dan
07/24/2012
Greg Steiner
07/24/2012
gary weider
07/25/2012
Greg Steiner
07/26/2012
Baker k. Vinci
07/27/2012
Carlos Boudet DDS
07/24/2012
Ä°lker Erdogan
07/25/2012
rsdds
07/25/2012
gary weider
07/25/2012
gary weider
07/25/2012
Baker k. Vinci
07/30/2012
james butler
07/25/2012
TMG
07/25/2012
gary weider
07/25/2012
TMG
07/26/2012
Dr. Alex Zavyalov
07/25/2012
Juan Rumeu
07/25/2012
Harris Mann
07/25/2012
gary weider
07/25/2012
gary
07/25/2012
Baker k. Vinci
07/26/2012
dr. bob
07/25/2012
dean tanaka
07/26/2012
CRS
08/07/2012
Carlo santos
09/04/2012
Featured Products
Classic 50/50 Mix
Promotes osteoconduction
Provides structural integrity
Convenient Syringe!
50/50 Cortical/Cancellous
Available in 3 sizes.
Eliminate hassle of mixing particulate grafts
Sold in packs of 5 or packs of 10.
Proven safe, and clinically effective
Resorbable collagen membrane derived from purified porcine pericardium
Fast hydration and excellent tensile strength
Good adaptation to various defects
Excellent tear function and duration
100% allograft
Eliminates mixing hassle
Moldable after hydration
Gregori M. Kurtzman, DDS,
07/24/2012