Fractured Upper Molar Case: Bone Regeneration and Sinus Lift
Last Updated: Jan 22, 2019
Case submitted by: Dr. Gerald Rudick with the assistance of Arta Prenga & Shlomit Dayan
Forty year old female in excellent health presented having pain in the upper right quadrant. Xray shows tooth #16 ( 3) had previous endodontics, post and core and a crown several years before and there is evidence of a root fracture….. the prognosis of keeping this tooth is hopeless (Fig. 1).
Following local anaesthesia , the tooth was extracted flaplessly with a conventional forceps. However, the apical portions of the two buccal roots separated. With a periosteal elevator, one of the broken roots was easily dislodged and removed, and the remaining root tip left and will be removed at the time of the bone grafting surgery. The patient was given antibiotics and analgesics and told to return in a month’s time so that some healing and detoxification of the socket can take place, as well as soft tissue closure. A full thickness flap was opened showing the amount of destruction that had occurred because of the apical pathology, and a clear view of the remaining root tip (Fig 2). It is important to note that unless successful bone regeneration can be accomplished to correct the defect, there is a strong possibility that the adjacent teeth will be lost.
Prior to opening the flap, 4 vials of blood were drawn in empty red capped tubes and spun in the centrifuge to obtain fibrin clots . The clots were then pressed to make membranes (Fig. 3).The fluid that was extruded from pressing the fibrin clots is Fibronectin and Vitreonectin, which is used as the wetting agents for the particulate graft mixture of Osteodemin, Allosorb and Osteogen, with a sprinkling of Metronidazol powder. The graft mixture is compacted into the defect and covered with the sticky fibrin membranes which are rich in growth factors. They also prevent the graft from being washed out (Fig .4 ).
A piece of titanium mesh is cut and folded to a saddle shape to fit over the graft site (Fig. 5). The titanium mesh was not screwed down , and it is covered with a piece of PTFE membrane to block the holes of the mesh while bone formation is taking place.The gingival mucosa was approximated as much as possible but because the area is bulked out it was not possible to get complete closure of the soft tissue. Gut sutures were used to secure the soft tissue (Fig.6).The disturbance to the soft tissue sets up RAP ( Regional Acceleratory Phenomenon), as described by Carl Misch some years ago, and this disturbance can speed up healing 2-3 times. The soft tissues will mend and close to a greater extent. As time goes by in the four month healing period, however, the titanium tends to become exposed and the PTFE that was covering the pores in the metal gets sloughed off….but new bone is growing under the titanium mesh, even though it is exposed. If the titanium becomes exposed, it could be annoying to the patient, however the irritating area of the mesh may be folded or cut off.
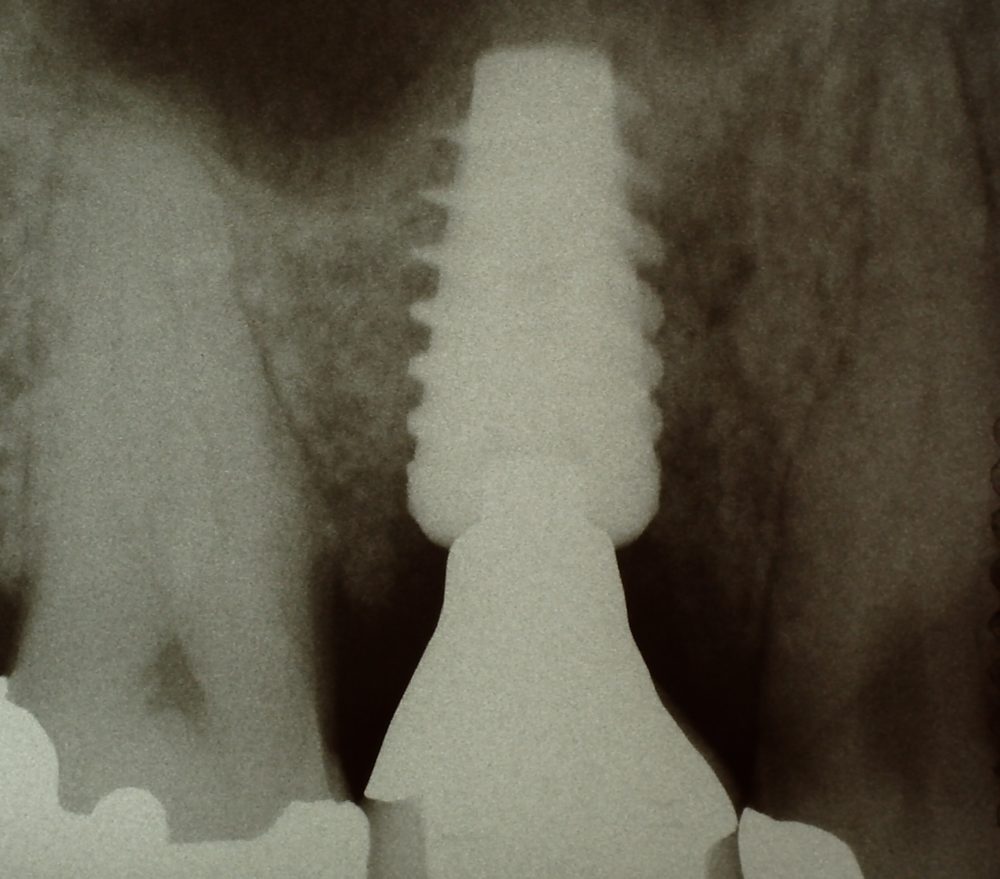
When the the four month healing period has expired (fig 7 ), the mesh which is completely immobile, is ready to be peeled off, (fig.8) revealing new bone that has developed, and the soft tissues are resutured giving complete closure. After another month or two allowing for further mineralization of the newly developed bone, an osteotomy is prepared in a closed technique, using conventional drills to the limited of the floor of the sinus, and with Osteotomes, the sinus membrane is lifted slightly,and a fibrin plug was placed in the hole with some grafting material, before the implant is screwed into place. ( fig. 9), which is evident in the xray. Waiting 3-4 months after implant placement, an impression is taken and a porcelain to metal screw retained crown is fabricated ( Figs. 10, 11).
Fig. 12 demonstrates the different steps that were taken. This case is now five years old, and is working out very well. It is important to note, that when the titanium is folded to a saddle shape, it is not necessary to screw it down, and is easier to remove when the healing period is completed.
 My beautiful picture
My beautiful picture







![]prognosis of keeping this tooth is hopeless](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2019/01/19579-24-10-c461962c473b-e1548108377916.jpg)prognosis of keeping this tooth is hopeless

prognosis){kind=link}
17 Comments on Fractured Upper Molar Case: Bone Regeneration and Sinus Lift
Dr. Gerald Rudick
01/22/2019
Andy
01/22/2019
Dr. Gerald Rudick
01/22/2019
Doc
01/22/2019
Dr. Gerald Rudick
01/22/2019
Yossi
01/23/2019
Dr. Gerald Rudick
01/23/2019
roadkingdoc
01/23/2019
Dr. Gerald Rudick
01/23/2019
DrK
01/25/2019
Dr. Gerald Rudick
01/25/2019
DrK
01/27/2019
roadkingdoc
01/27/2019
Dr. Gerald Rudick
01/28/2019
roadkingdoc
01/28/2019
Dr. Gerald Rudick
01/28/2019
Featured Products
Classic 50/50 Mix
Promotes osteoconduction
Provides structural integrity
Convenient Syringe!
50/50 Cortical/Cancellous
Available in 3 sizes.
Eliminate hassle of mixing particulate grafts
Sold in packs of 5 or packs of 10.
Proven safe, and clinically effective
Resorbable collagen membrane derived from purified porcine pericardium
Fast hydration and excellent tensile strength
Good adaptation to various defects
Excellent tear function and duration
100% allograft
Eliminates mixing hassle
Moldable after hydration
Dr Dale Gerke, BDS, BScDe
01/22/2019