Retained Root Tip in the Sinus: How To Proceed with Dental Implant Placement?
Last Updated: May 13, 2012
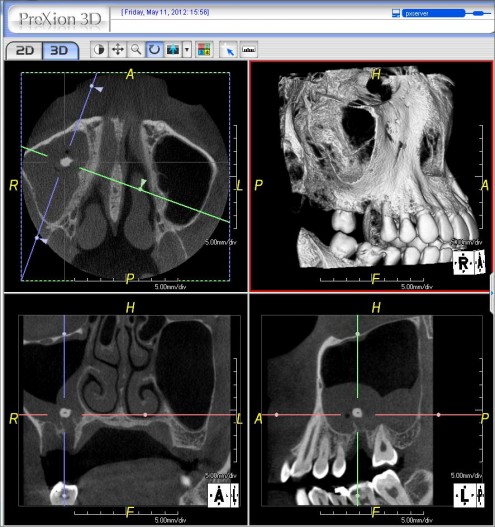
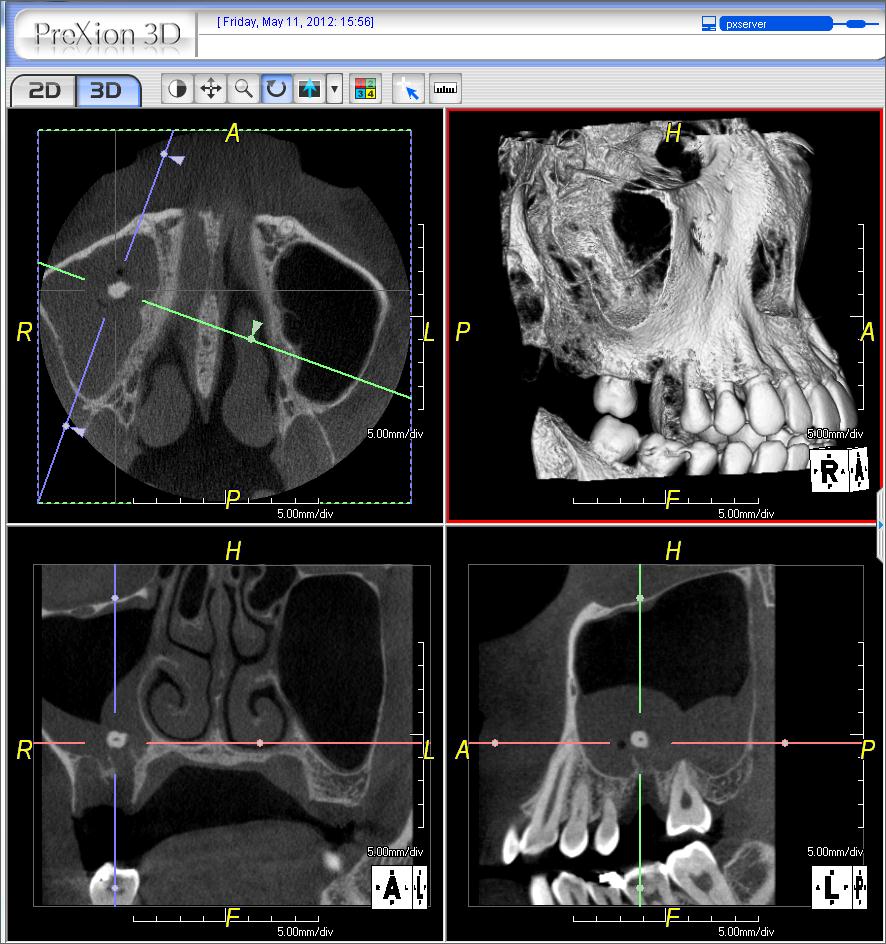
I am a periodontist and recently had a case referred for installation of a dental implant in #3 area [maxillary right first molar; 16]. Â The patient had #3 extracted 2 weeks prior and there is a root tip — probably from the palatal root — in the maxillary sinus. Â This is clearly visible in the CBVT scan. There is also an apparent oral antral fistula between the maxillary sinus and the oral cavity. Â I prescribed Biaxin [clarithromycin]. What is the recommended course of treatment to manage the root tip and graft the area for a future implant? How do you recommend I proceed? Â
(click image to enlarge)
![]retained root tip in sinus](https://osseonews.nyc3.cdn.digitaloceanspaces.com/wp-content/uploads/2012/05/Root-tip-in-the-sinus.jpeg)
{kind=link}
{kind=link}
45 Comments on Retained Root Tip in the Sinus: How To Proceed with Dental Implant Placement?
Baker vinci
05/16/2012
Leal
05/16/2012
Baker vinci
05/16/2012
Gregori M. Kurtzman, DDS,
05/16/2012
David Nelson DDS
05/18/2012
Guy Carnazza DMD
05/14/2012
Baker vinci
05/17/2012
Baker vinci
05/18/2012
Gregori M. Kurtzman, DDS,
06/28/2012
Greg Steiner
05/14/2012
Baker vinci
05/21/2012
Levon Galstyan, MD, DMD,
06/28/2012
Levon Galstyan, MD, DMD,
06/28/2012
Gregori M. Kurtzman, DDS,
05/14/2012
Dorian Hatchuel
05/15/2012
CRS
05/15/2012
Baker vinci
05/16/2012
Peter McKenna
05/15/2012
Cristian Lagos
05/15/2012
Dr. dan
05/15/2012
Vipul G Shukla
05/15/2012
osurg
05/15/2012
Baker vinci
05/16/2012
TW
05/15/2012
SBoral surgeon
05/15/2012
SBoral surgeon
05/15/2012
Baker vinci
05/16/2012
Gregori M. Kurtzman, DDS,
06/28/2012
Baker vinci
05/16/2012
Baker vinci
05/16/2012
Dr BJ
05/16/2012
Baker vinci
05/17/2012
peter fairbairn
05/17/2012
Dr Campos
05/17/2012
Art Greenwald
05/17/2012
DR S
05/18/2012
DrOMS
05/19/2012
Richard Hughes, DDS, FAAI
05/20/2012
Jace
05/20/2012
Gregori M. Kurtzman, DDS,
05/20/2012
Allen ong
05/23/2012
CRS
06/05/2012
CRS
06/05/2012
Shd
06/19/2012
Featured Products
Classic 50/50 Mix
Promotes osteoconduction
Provides structural integrity
Convenient Syringe!
50/50 Cortical/Cancellous
Available in 3 sizes.
Eliminate hassle of mixing particulate grafts
Sold in packs of 5 or packs of 10.
Proven safe, and clinically effective
Resorbable collagen membrane derived from purified porcine pericardium
Fast hydration and excellent tensile strength
Good adaptation to various defects
Excellent tear function and duration
100% allograft
Eliminates mixing hassle
Moldable after hydration
Leal
05/13/2012