I do implant and ortho treatment regularly. I disagree with doing ortho treatment in this 53 yrs pt that has some periodontal issue. Uprighting the last Mandibular molars in this case might cause both of them to be in worse prognosis - we might end up loosing them. So it's better to work with this situation as it is.
I will just shave the premolar crown (#13/25) since it has RCT already.
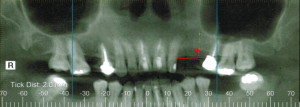
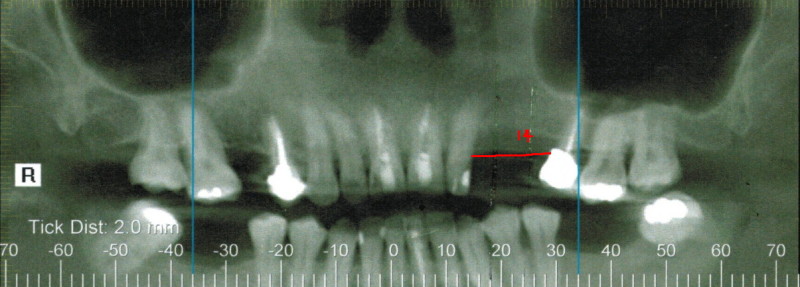
At the last slice of CT you see radiolucency at the apex, so this tooth might need implant in the near future. I will not put the new crown because of it's guided prognosis. I will then put 1 implant on # 12/24 area and restore it with cantilever 2 unit bridge on the mesial (canine). It's easier than placing 2 narrow implant. I had several cases like this and I found out that it is very difficult to restore the canine in good relation to lateral incisor, maybe because the angle of lateral is protruding more due to collapse of occlusion / perio problem. But I will maximize the size of the implant, from the CT Scan it show that we can use 4.5 or even 5.0 width of implant.
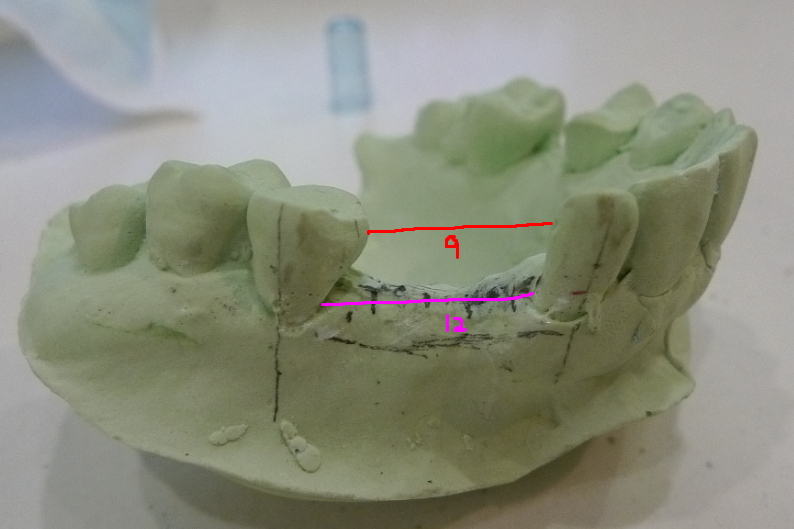
For the lower arch, it's better to restore the edentulous sites with implant as well or at least partial denture. I personally will not even consider placing implant on the upper arch just for esthetic( if pt is unwilling to pay for lower partial denture ), because functionally the implant will be overloaded. Ideally, I will suggest the patient to use Valplast or stay plate on the upper arch and placing implant on lower molars first before placing implant on the upper arch. At least I will fabricate a good lower partial denture before I restore the cantilever bridge on # 11/12 ( 23/24). Functional first then esthetic second - this I always try to emphasis, especially dealing with middle age women.
Implant is not for everyone. If pt has limited financial problem, I will just restore the upper arch with Valplast & that will be it. Otherwise you will risk yourself to deal with broken screw or post, no matter what kind of implant you will use. Think 1 or 2 steps ahead of the game ( like in the chess). If # 13/25 need to be extracted after you place implant(s) next to it, it will be really bad situation. Then you'll make her problem to be your problem.
sharon
6/24/2014
Hi Andy; I like your response in a difficult case like this. If you were to place an implant in #19 position how would you manage the opposing #14? if you were going to cantilever a pontic #11 from #12 would you keep the pontic out of lateral excursion to avoid lateral forces on it? I guess if there is an apical rae on #13 the sensible thing to do before placing an implant #14 is to redo RCT? Thank you!!
Andy K
7/4/2014
Many implant cases are not straight forward deal. Often we need to compromise the perfect result and live with acceptable condition.
If I want to restore #19, I will burry my implant deeper. That's why I love Bicon, because I can do modification with implant as short as 5 mm. The future crown # 19 will be little inferior than # 18/20. Then I will do enameloplasty on # 14 & if necessary crown, but I will try not to do RCT on it. With other implant system, most likely I will need to perform RCT on # 14.
Once we have implant on #19, restoring # 11/12 is easier. Yes, I will keep the Pontic out of lateral excursion force. In this 11/12, I will not use Bicon, because it will get loose easily. I will use screw type of implant.














{kind=link}
conebeam){kind=link}
{kind=link}
model){kind=link}
{kind=link}
cone){kind=link}
{kind=link}
e){kind=link}
{kind=link}
model){kind=link}